Yang Jin, Cao Yuying, Zhou Fangzhu, Li Chengyao, Lv Jiabei, Li Pu
Clinical School of Obstetrics and Gynecology Center, Tianjin Medical University, Tianjin, China.
Front Oncol. 2023 Oct 16;13:1231497. doi: 10.3389/fonc.2023.1231497. eCollection 2023.
Differences exist between high- and low-risk endometrial cancer (EC) in terms of whether lymph node dissection is performed. Factors such as tumor grade, myometrial invasion (MDI), and lymphovascular space invasion (LVSI) in the European Society for Medical Oncology (ESMO), European SocieTy for Radiotherapy & Oncology (ESTRO) and European Society of Gynaecological Oncology (ESGO) guidelines risk classification can often only be accurately assessed postoperatively. The aim of our study was to estimate the risk classification of patients with endometrial endometrioid adenocarcinoma before surgery and offer individualized treatment plans based on their risk classification.
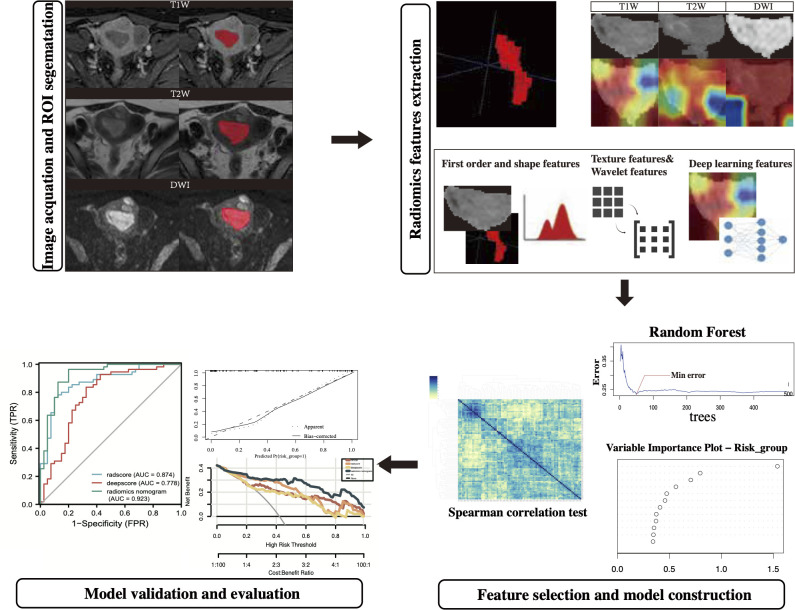
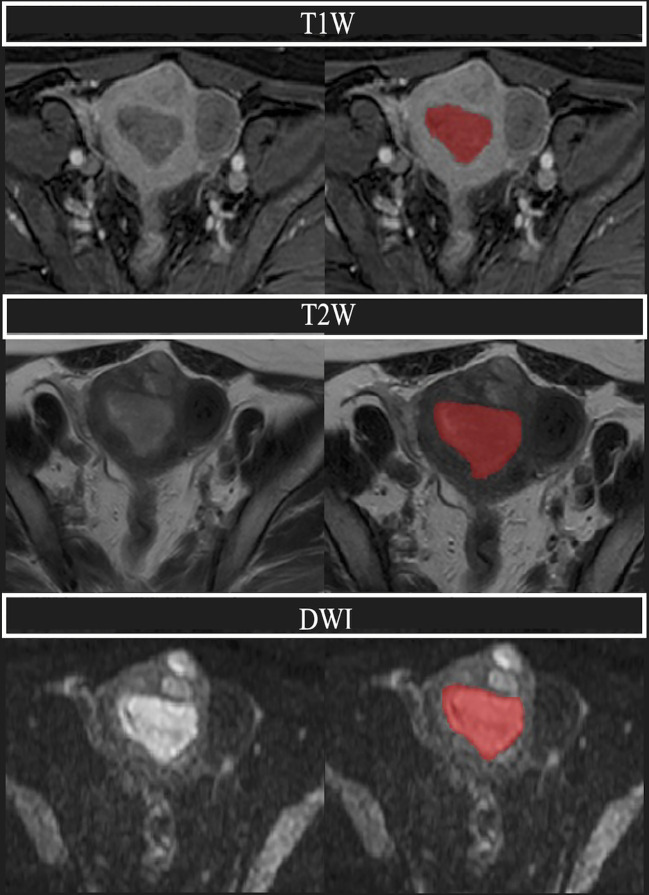
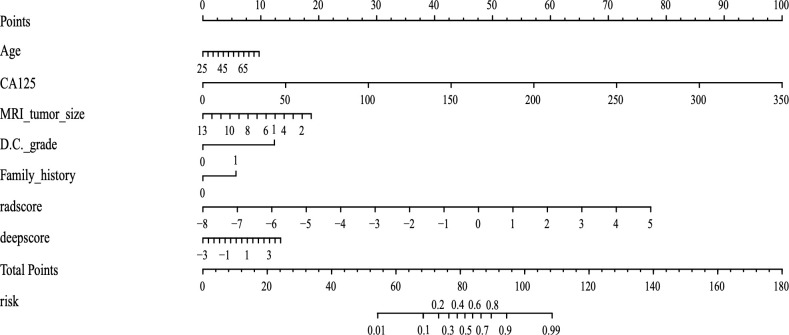
Clinical information and last preoperative pelvic magnetic resonance imaging (MRI) of patients with postoperative pathologically determined endometrial endometrioid adenocarcinoma were collected retrospectively. The region of interest (ROI) was subsequently plotted in T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), and diffusion-weighted imaging (DWI) MRI scans, and the traditional radiomics features and deep-learning image features were extracted. A final radiomics nomogram model integrating traditional radiomics features, deep learning image features, and clinical information was constructed to distinguish between low- and high-risk patients (based on the 2020 ESMO-ESGO-ESTRO guidelines). The efficacy of the model was evaluated in the training and validation sets of the model.
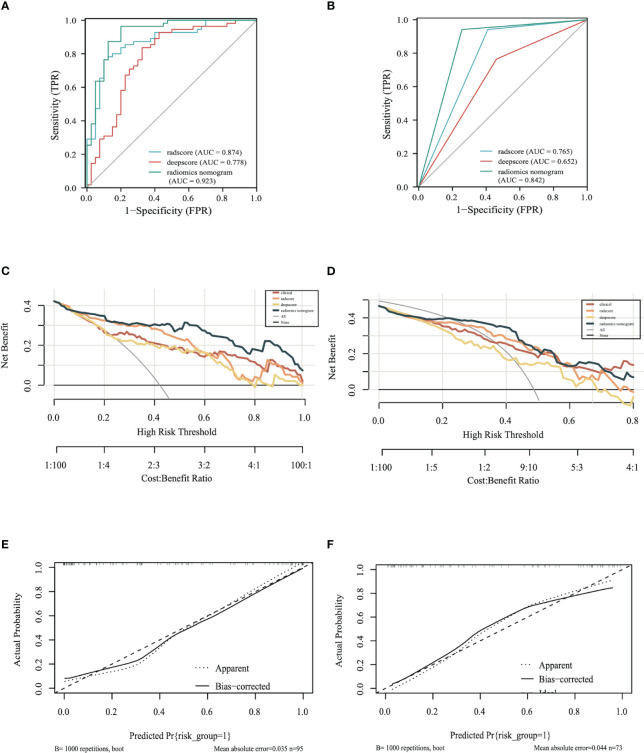
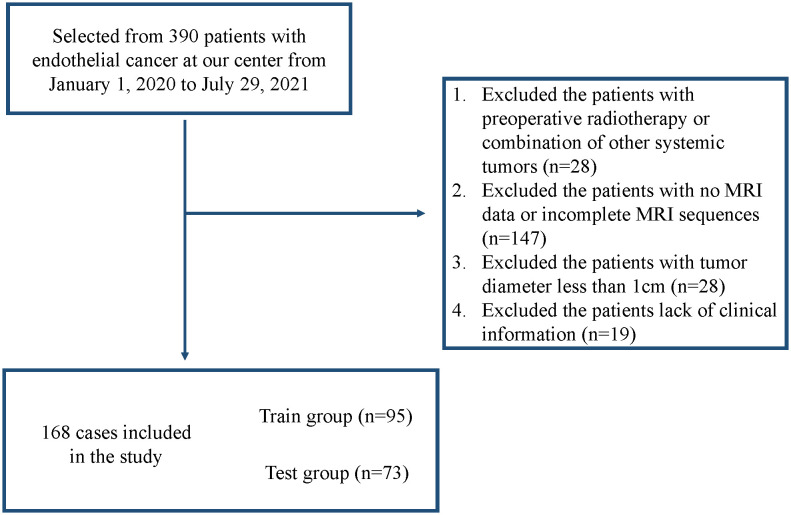
We finally included 168 patients from January 1, 2020 to July 29, 2021, of which 95 patients in 2021 were classified as the training set and 73 patients in 2020 were classified as the validation set. In the training set, the area under the curve (AUC) of the radiomics nomogram was 0.923 (95%CI: 0.865-0.980) and in the validation set, the AUC of the radiomics nomogram was 0.842 (95%CI: 0.762-0.923). The nomogram had better predictions than both the traditional radiomics model and the deep-learning radiomics model.
MRI-based radiomics models can be useful for preoperative risk classification of patients with endometrial endometrioid adenocarcinoma.
在是否进行淋巴结清扫方面,高风险和低风险子宫内膜癌(EC)存在差异。欧洲医学肿瘤学会(ESMO)、欧洲放射治疗与肿瘤学会(ESTRO)和欧洲妇科肿瘤学会(ESGO)指南中的风险分类所涉及的因素,如肿瘤分级、肌层浸润(MDI)和脉管间隙浸润(LVSI),通常只能在术后准确评估。我们研究的目的是在手术前评估子宫内膜样腺癌患者的风险分类,并根据其风险分类提供个性化治疗方案。
回顾性收集术后病理确诊为子宫内膜样腺癌患者的临床信息和术前最后一次盆腔磁共振成像(MRI)。随后在T1加权成像(T1WI)、T2加权成像(T2WI)和扩散加权成像(DWI)MRI扫描中绘制感兴趣区域(ROI),并提取传统放射组学特征和深度学习图像特征。构建一个整合传统放射组学特征,并提取深度学习图像特征和临床信息的最终放射组学列线图模型,以区分低风险和高风险患者(基于2020年ESMO-ESGO-ESTRO指南)。在模型的训练集和验证集中评估该模型的有效性。
我们最终纳入了2020年1月1日至2021年7月29日的168例患者,其中2021年的95例患者被分类为训练集,2020年的73例患者被分类为验证集。在训练集中,放射组学列线图的曲线下面积(AUC)为0.923(95%CI:0.865-0.980),在验证集中,放射组学列线图的AUC为0.842(95%CI:0.762-0.923)。该列线图的预测效果优于传统放射组学模型和深度学习放射组学模型。
基于MRI的放射组学模型可用于子宫内膜样腺癌患者的术前风险分类。