Program on Regulation, Therapeutics, and Law (PORTAL), Division of Pharmacoepidemiology and Pharmacoeconomics, Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2023 Nov 1;6(11):e2343285. doi: 10.1001/jamanetworkopen.2023.43285.
Many cancer drugs are approved under the US Food and Drug Administration (FDA) accelerated approval pathway based on preliminary evidence. It is unclear how this limited evidence is integrated into the National Comprehensive Cancer Network (NCCN) guidelines, which are common references for clinicians and are used by public and private payers to determine reimbursement for oncology treatments.
To analyze the NCCN guidelines' assessments for cancer drug indications that received FDA accelerated approval compared with cancer drug indications that received FDA regular approval.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study analyzes FDA-approved indications for cancer drugs that were granted accelerated approval from program inception in 1992 to June 30, 2022. For each drug, the FDA-approved labeling was reviewed to identify all indications. All analyses were performed at the drug-indication level.
The exposure was FDA regulatory status as of October 2022, including regular approval, accelerated approval, accelerated approval converted to regular approval, and withdrawn accelerated approval.
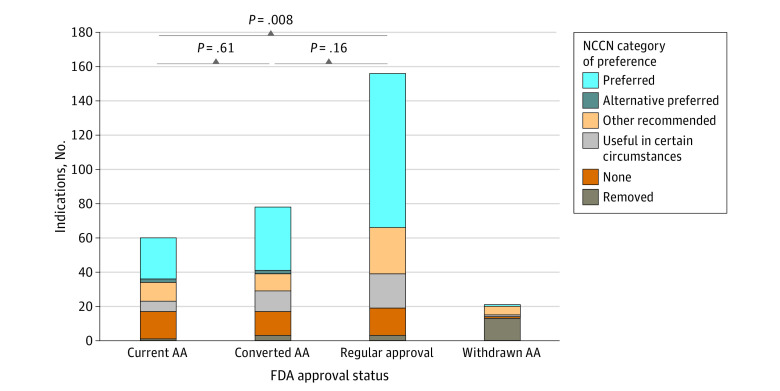
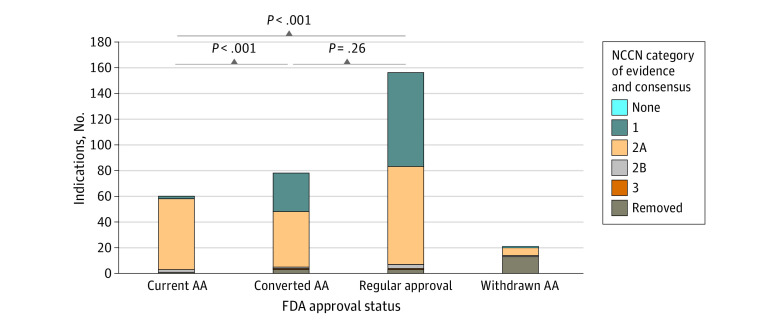
The level of evidence and consensus (category 1, 2A, 2B, and 3) and treatment preference (preferred, alternative preferred, other recommended, and useful in certain circumstances) ratings assigned by NCCN committees as of February 2023.
A total of 315 oncology indications for 100 drugs were analyzed. These indications included 156 (50%) with regular approval, 60 (38%) with accelerated approval, 78 (49%) with accelerated approval that was converted to regular approval, and 21 (13%) with withdrawn accelerated approvals. Among all indications, 105 (33%) were rated by the NCCN as having category 1 evidence, 185 (59%) with category 2A, 6 (2%) with category 2B, and 2 (1%) with category 3 evidence. Compared with indications with regular approval, those with accelerated approval were less frequently assigned category 1 evidence (47% vs 3%; P < .001) and were less often listed as preferred treatment options (58% vs 40%; P = .008). Among the 21 withdrawn accelerated approval indications, 8 (38%) remained in the NCCN guidelines, with most having level 2A evidence ratings.
This study found that cancer drug indications with accelerated approval were less likely to be assigned high-level evidence ratings and preferred status in the NCCN guidelines compared with indications with regular approval; most accelerated and regular approval drugs had low-quality evidence ratings but high levels of consensus among oncologists on NCCN committees. Greater clarity on the thresholds and definitions of evidence levels would make the NCCN guidelines more useful to clinicians, patients, and payers.
许多癌症药物是根据美国食品和药物管理局(FDA)的加速批准途径获得批准的,依据的是初步证据。目前尚不清楚如何将这些有限的证据纳入国家综合癌症网络(NCCN)指南,NCCN 指南是临床医生的常用参考依据,公共和私人支付方也会利用这些指南来确定癌症治疗的报销范围。
分析 NCCN 指南中对接受 FDA 加速批准的癌症药物适应证的评估与接受 FDA 常规批准的癌症药物适应证的评估。
设计、设置和参与者:这项横断面研究分析了自 1992 年该项目启动至 2022 年 6 月 30 日获得 FDA 加速批准的癌症药物适应证。对每种药物,均对 FDA 批准的标签进行了审查,以确定所有适应证。所有分析均在药物-适应证水平进行。
截至 2022 年 10 月,暴露情况为 FDA 的监管状况,包括常规批准、加速批准、加速批准转换为常规批准和撤回的加速批准。
截至 2023 年 2 月,NCCN 委员会分配的证据水平和共识(类别 1、2A、2B 和 3)以及治疗偏好(首选、首选替代、其他推荐和在某些情况下有用)评级。
共分析了 100 种药物的 315 个肿瘤适应证。这些适应证包括 156 个(50%)为常规批准适应证,60 个(38%)为加速批准适应证,78 个(49%)为加速批准适应证转换为常规批准适应证,21 个(13%)为撤回的加速批准适应证。在所有适应证中,有 105 个(33%)被 NCCN 评为类别 1 证据,185 个(59%)为类别 2A,6 个(2%)为类别 2B,2 个(1%)为类别 3 证据。与常规批准适应证相比,加速批准适应证不太可能被分配类别 1 证据(47%比 3%;P<0.001),也不太可能被列为首选治疗方案(58%比 40%;P=0.008)。在 21 个撤回的加速批准适应证中,有 8 个(38%)仍在 NCCN 指南中,其中大多数具有 2A 类证据评级。
这项研究发现,与常规批准适应证相比,接受加速批准的癌症药物适应证更不可能在 NCCN 指南中被分配到高级别证据评级和首选治疗方案地位;大多数加速和常规批准药物的证据评级质量较低,但肿瘤学家在 NCCN 委员会中的共识水平较高。更明确证据水平的阈值和定义将使 NCCN 指南对临床医生、患者和支付方更有用。