Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), Nuffield Department of Population Health, University of Oxford, Oxford, UK.
Cancer Epidemiology Unit (CEU), Nuffield Department of Population Health, University of Oxford, Oxford, UK.
BMC Med. 2023 Nov 16;21(1):444. doi: 10.1186/s12916-023-03135-8.
Excess energy intake can lead to metabolic dysfunction-associated steatotic liver disease (MASLD), but the relationship between dietary carbohydrate intake and liver fat content remains unclear. This study aimed to examine the associations between types and sources of dietary carbohydrates and liver fat content.
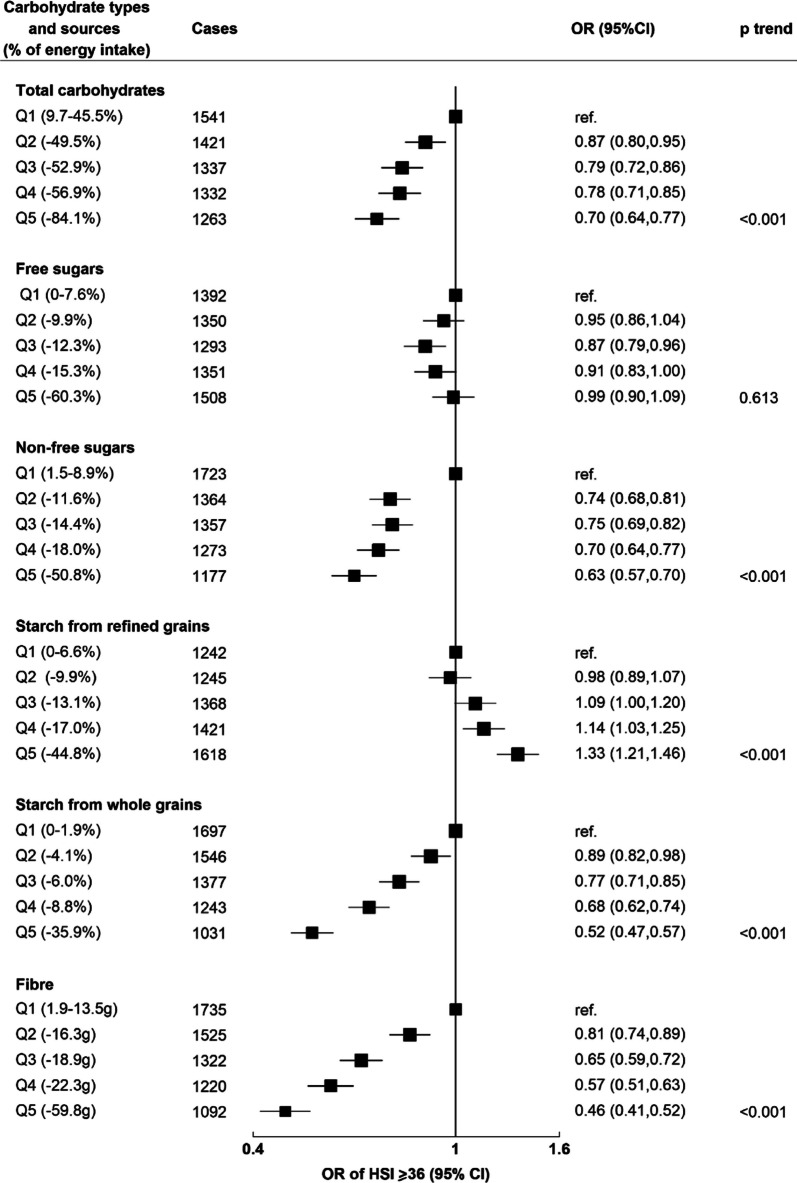
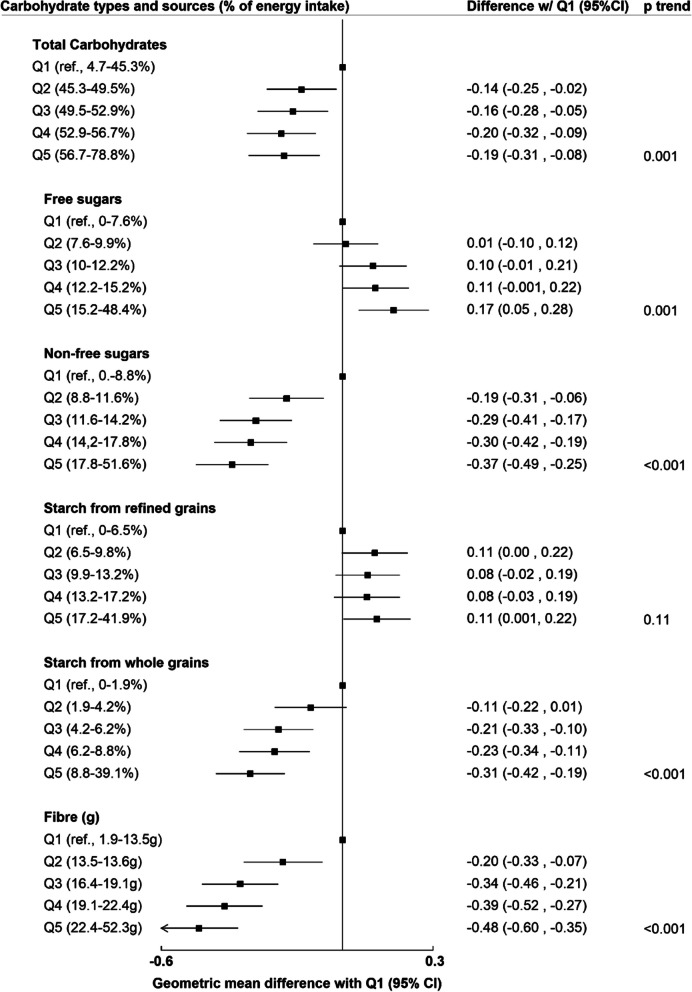
UK Biobank participants with no pre-existing diabetes, liver disease or cardiovascular disease reported dietary intake of types and sources of carbohydrates (total carbohydrates, free sugars, non-free sugars, starch from whole grains, starch from refined grains, and fibre) on at least two 24-h dietary assessments. In cross-sectional analyses, (n = 22,973), odds ratios (OR) of high liver fat content (defined as a score of ≥ 36 in the hepatic steatosis index) by quintiles of carbohydrate intakes were estimated using multivariable logistic regression models. In prospective analyses, a second sample (n = 9268) had liver proton density fat fraction (PDFF) measured by magnetic resonance imaging (2014-2020). Multivariable linear regression models estimated geometric means of PDFF (%) by quintiles of carbohydrate intakes. Models were adjusted for demographic and lifestyle confounders, including total energy intake.
In the cross-sectional analyses, 6894 cases of high liver fat content were identified. Inverse associations between intakes of fibre (OR of highest vs. lowest quintile 0.46 [95% CI: 0.41-0.52]), non-free sugars (0.63 [0.57-0.70]) and starch from whole grains (0.52 [0.47-0.57]) with liver fat were observed. There were positive associations between starch from refined grains and liver fat (1.33 [1.21-1.46]), but no association with free sugars (p=0.61). In prospective analyses, inverse associations with PDFF (%) were observed for intakes of fibre (- 0.48 geometric mean difference between highest and lowest quintile of intake [- 0.60 to - 0.35]), non-free sugars (- 0.37 [- 0.49 to - 0.25]) and starch from whole grains (- 0.31 [- 0.42 to - 0.19]). Free sugars, but not starch from refined grains, were positively associated with PDFF (0.17 [0.05 to 0.28]).
This study suggests that different carbohydrate types and sources have varying associations with liver fat, which may be important for MASLD prevention. Non-free sugars, fibre, and starch from whole grains could be protective, while associations with free sugars and starch from refined grains are less clear.
摄入过多能量会导致代谢功能障碍相关的脂肪性肝病(MASLD),但饮食中碳水化合物的摄入量与肝脂肪含量之间的关系尚不清楚。本研究旨在研究不同类型和来源的碳水化合物与肝脂肪含量之间的关系。
英国生物库中没有糖尿病、肝病或心血管疾病的参与者报告了至少两次 24 小时饮食评估中碳水化合物的类型和来源(总碳水化合物、游离糖、非游离糖、全麦淀粉、精制谷物淀粉和纤维)的摄入量。在横断面分析中(n=22973),使用多变量逻辑回归模型估计了肝脂肪含量高(肝脂肪指数评分≥36)的五分位数碳水化合物摄入量的比值比(OR)。在前瞻性分析中,第二个样本(n=9268)通过磁共振成像(2014-2020 年)测量了肝质子密度脂肪分数(PDFF)。多变量线性回归模型估计了碳水化合物摄入量五分位数的 PDFF(%)的几何平均值。模型调整了包括总能量摄入在内的人口统计学和生活方式混杂因素。
在横断面分析中,确定了 6894 例肝脂肪含量高的病例。纤维摄入量(最高五分位数与最低五分位数的比值比 0.46 [95%CI:0.41-0.52])、非游离糖(0.63 [0.57-0.70])和全麦淀粉(0.52 [0.47-0.57])与肝脂肪呈负相关。精制谷物淀粉与肝脂肪呈正相关(1.33 [1.21-1.46]),但游离糖无关联(p=0.61)。在前瞻性分析中,纤维摄入量(最高五分位数与最低五分位数之间的 PDFF(%)的几何平均差异为-0.48[摄入的-0.60 至-0.35])、非游离糖(-0.37[-0.49 至-0.25])和全麦淀粉(-0.31[-0.42 至-0.19])与 PDFF 呈负相关。游离糖(0.17 [0.05 至 0.28]),而不是精制谷物淀粉,与 PDFF 呈正相关。
本研究表明,不同类型和来源的碳水化合物与肝脂肪含量有不同的关系,这对 MASLD 的预防可能很重要。非游离糖、纤维和全麦淀粉可能具有保护作用,而游离糖和精制谷物淀粉的关联则不太明确。