Division of Perioperative Informatics, Department of Anesthesiology, University of California San Diego, 9300 Campus Point Drive, MC7770, La Jolla, CA, 92037-7770, USA.
School of Medicine, University of California San Diego, 9500 Gilman Dr, La Jolla, CA, 92093, USA.
J Med Syst. 2023 Nov 16;47(1):119. doi: 10.1007/s10916-023-02015-1.
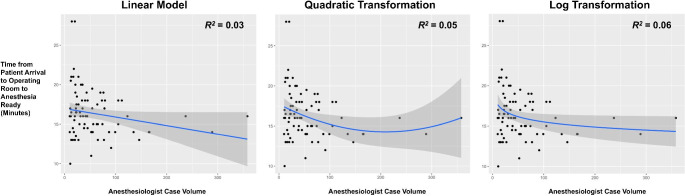
The objective of this retrospective study was to determine if there was an association between anesthesiology experience (e.g. historic case volume) and operating room (OR) efficiency times for lower extremity joint arthroplasty cases. The primary outcome was time from patient in the OR to anesthesia ready (i.e. after spinal or general anesthesia induction was complete). The secondary outcomes included time from anesthesia ready to surgical incision, and time from incision to closing completed. Mixed effects linear regression was performed, in which the random effect was the anesthesiology attending provider. There were 4,575 patients undergoing hip or knee arthroplasty included. There were 82 unique anesthesiology providers, in which the median [quartile] frequency of cases performed was 79 [45, 165]. On multivariable mixed effects linear regression - in which the primary independent variable (anesthesiologist case volume history for joint arthroplasty anesthesia) was log-transformed - the estimate for log-transformed case volume was - 0.91 (95% confidence interval [CI] -1.62, -0.20, P = 0.01). When modeling time from incision to closure complete, the estimate for log-transformed case volume was - 2.07 (95% -3.54, -0.06, P = 0.01). Thus, when comparing anesthesiologists with median case volume (79 cases) versus those with the lowest case volume (10 cases), the predicted difference in times added up to only approximately 6 min. If the purpose of faster anesthesia workflows was to open up more OR time to increase surgical volume in a given day, this study does not support the supposition that anesthesiologists with higher joint arthroplasty case volume would improve throughput.
这项回顾性研究的目的是确定麻醉科经验(例如历史病例量)与下肢关节置换术病例手术室(OR)效率时间之间是否存在关联。主要结果是患者进入 OR 到麻醉准备(即脊髓或全身麻醉诱导完成后)的时间。次要结果包括从麻醉准备到手术切口的时间,以及从切口到完成缝合的时间。进行了混合效应线性回归,其中随机效应是麻醉科主治医生。共有 4575 名接受髋关节或膝关节置换术的患者纳入研究。共有 82 名独特的麻醉科医生,其中中位数[四分位数]手术频率为 79[45,165]。在多变量混合效应线性回归中,主要自变量(关节置换麻醉的麻醉师病例量历史)进行了对数转换,对数转换病例量的估计值为-0.91(95%置信区间[CI] -1.62,-0.20,P=0.01)。在从切口到完成缝合的时间模型中,对数转换病例量的估计值为-2.07(95%CI-3.54,-0.06,P=0.01)。因此,当比较中位数病例量(79 例)和最低病例量(10 例)的麻醉师时,预计时间差异仅增加约 6 分钟。如果加快麻醉工作流程的目的是开放更多的 OR 时间来增加给定一天的手术量,那么本研究不支持这样的假设,即具有更高关节置换病例量的麻醉师将提高吞吐量。