Division of Digestive Surgery, Department of Surgery, Geneva University Hospital and Faculty of Medicine, Geneva, Switzerland.
Department of Surgery and Transplantation, University Hospital Zurich, University of Zurich, Zurich, Switzerland.
Br J Surg. 2024 Jan 3;111(1). doi: 10.1093/bjs/znad374.
Whether the benefits of the robotic platform in bariatric surgery translate into superior surgical outcomes remains unclear. The aim of this retrospective study was to establish the 'best possible' outcomes for robotic bariatric surgery and compare them with the established laparoscopic benchmarks.
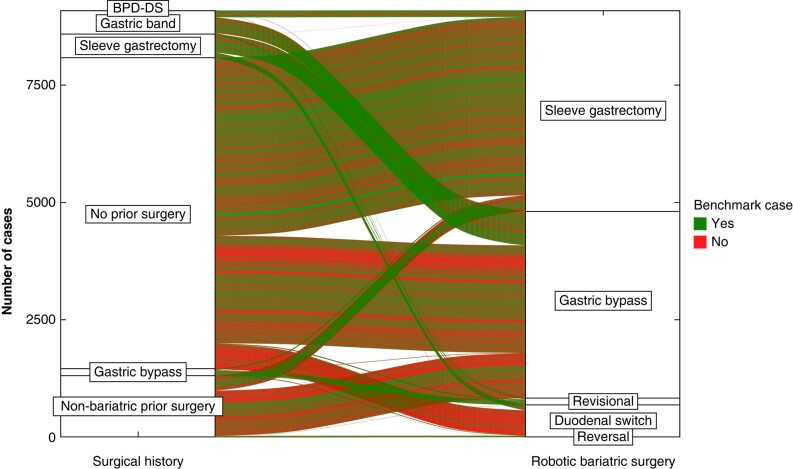
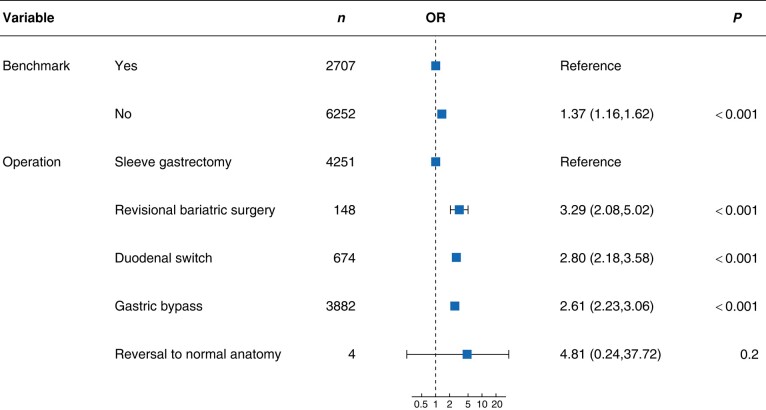
Benchmark cut-offs were established for consecutive primary robotic bariatric surgery patients of 17 centres across four continents (13 expert centres and 4 learning phase centres) using the 75th percentile of the median outcome values until 90 days after surgery. The benchmark patients had no previous laparotomy, diabetes, sleep apnoea, cardiopathy, renal insufficiency, inflammatory bowel disease, immunosuppression, history of thromboembolic events, BMI greater than 50 kg/m2, or age greater than 65 years.
A total of 9097 patients were included, who were mainly female (75.5%) and who had a mean(s.d.) age of 44.7(11.5) years and a mean(s.d.) baseline BMI of 44.6(7.7) kg/m2. In expert centres, 13.74% of the 3020 patients who underwent primary robotic Roux-en-Y gastric bypass and 5.9% of the 4078 patients who underwent primary robotic sleeve gastrectomy presented with greater than or equal to one complication within 90 postoperative days. No patient died and 1.1% of patients had adverse events related to the robotic platform. When compared with laparoscopic benchmarks, robotic Roux-en-Y gastric bypass had lower benchmark cut-offs for hospital stay, postoperative bleeding, and marginal ulceration, but the duration of the operation was 42 min longer. For most surgical outcomes, robotic sleeve gastrectomy outperformed laparoscopic sleeve gastrectomy with a comparable duration of the operation. In robotic learning phase centres, outcomes were within the established benchmarks only for low-risk robotic Roux-en-Y gastric bypass.
The newly established benchmarks suggest that robotic bariatric surgery may enhance surgical safety compared with laparoscopic bariatric surgery; however, the duration of the operation for robotic Roux-en-Y gastric bypass is longer.
机器人平台在减重手术中的益处是否能转化为更好的手术结果尚不清楚。本回顾性研究的目的是确定机器人减重手术的“最佳”结果,并将其与已确立的腹腔镜基准进行比较。
使用中位数结果值的第 75 个百分位数,在四个大陆的 17 个中心(13 个专家中心和 4 个学习阶段中心)对连续的原发性机器人减重手术患者进行基准截止值的建立,直到术后 90 天。基准患者没有既往剖腹手术、糖尿病、睡眠呼吸暂停、心脏病、肾功能不全、炎症性肠病、免疫抑制、血栓栓塞事件史、BMI 大于 50kg/m2 或年龄大于 65 岁。
共纳入 9097 例患者,主要为女性(75.5%),平均(标准差)年龄为 44.7(11.5)岁,平均(标准差)基线 BMI 为 44.6(7.7)kg/m2。在专家中心,3020 例接受原发性机器人 Roux-en-Y 胃旁路术的患者中,有 13.74%在术后 90 天内出现 1 种或以上并发症,4078 例接受原发性机器人袖状胃切除术的患者中,有 5.9%出现 1 种或以上并发症。无患者死亡,1.1%的患者出现与机器人平台相关的不良事件。与腹腔镜基准相比,机器人 Roux-en-Y 胃旁路术的住院时间、术后出血和边缘性溃疡的基准截止值较低,但手术时间长 42 分钟。对于大多数手术结果,机器人袖状胃切除术的手术效果优于腹腔镜袖状胃切除术,且手术时间相当。在机器人学习阶段中心,仅低风险的机器人 Roux-en-Y 胃旁路术的结果在既定基准内。
新确立的基准表明,与腹腔镜减重手术相比,机器人减重手术可能提高手术安全性;然而,机器人 Roux-en-Y 胃旁路术的手术时间较长。