Takahashi Goro, Matsuda Akihisa, Yamada Takeshi, Uehara Kay, Shinji Seiichi, Yokoyama Yasuyuki, Iwai Takuma, Takeda Kohki, Kuriyama Sho, Miyasaka Toshimitsu, Kanaka Shintaro, Terayachi Tai, Okino Tetsuya, Yoshida Hiroshi
Department of Gastrointestinal and Hepato-Biliary-Pancreatic Surgery, Nippon Medical School Hospital, Tokyo, 113-8603, Japan.
Surg Case Rep. 2023 Nov 21;9(1):201. doi: 10.1186/s40792-023-01784-8.
A colovesical fistula (CVF) is commonly treated by resection of the intestine containing the fistula or creation of a defunctioning stoma. We herein report a case of successful fistula closure and avoidance of colostomy after placement of a covered colonic self-expanding metallic stent (SEMS) as a palliative treatment for a malignant CVF.
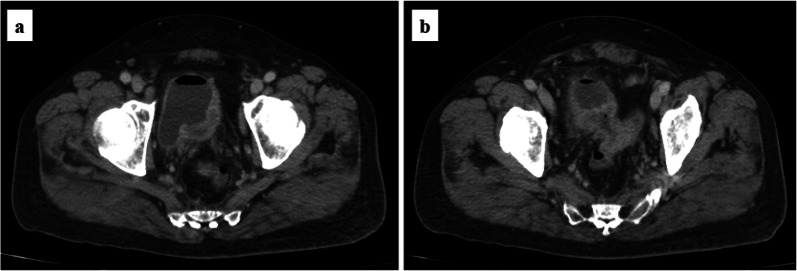
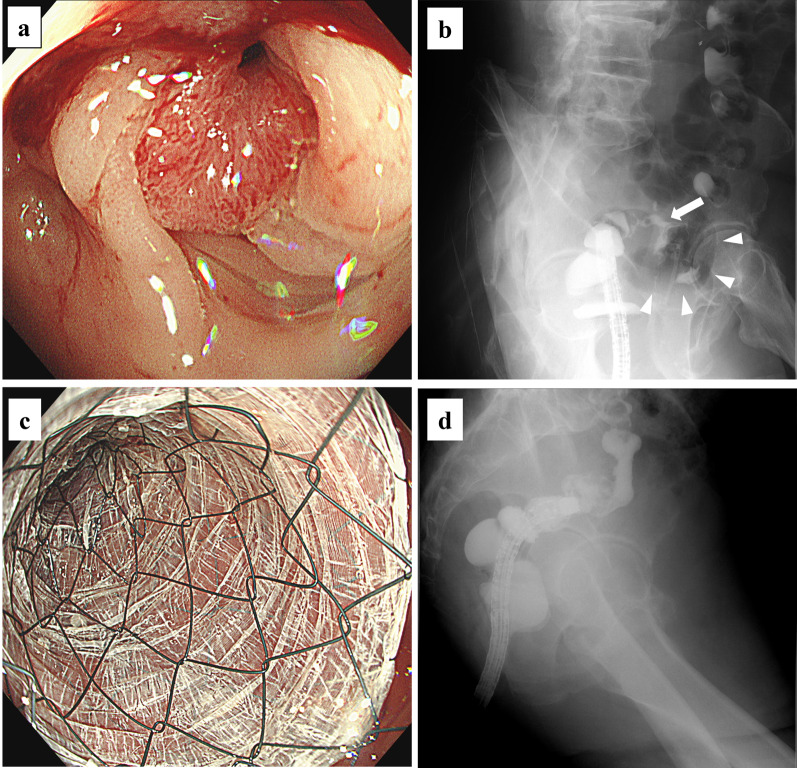
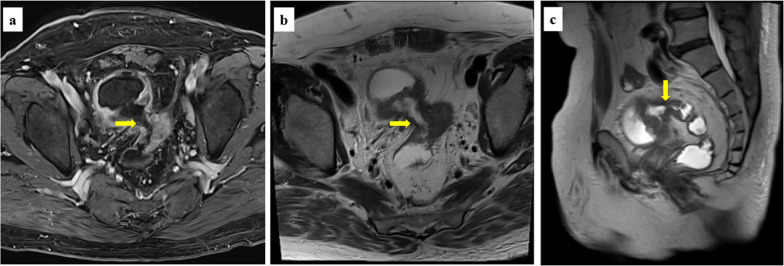
A 75-year-old man undergoing infusional 5-fluorouracil and irinotecan chemotherapy plus bevacizumab for recurrent peritoneal dissemination of rectal cancer was admitted to our hospital because of fecaluria with a high-grade fever. Blood tests showed a moderate inflammatory reaction (white blood cell count, 9200/mm; C-reactive protein, 11.03 mg/dL; procalcitonin, 1.33 ng/mL). Urinary sediment examination showed severe bacteriuria. Abdominal contrast-enhanced computed tomography showed intravesical gas, thickening of the posterior wall of the bladder, and irregular thickening of the sigmoid colon wall contiguous with the posterior bladder wall. Magnetic resonance imaging (MRI) clearly showed a fistula between the bladder and sigmoid colon. Colonoscopy revealed a circumferential malignant stricture 15 cm from the anal verge, and a fistula to the bladder was identified by water-soluble contrast medium. We diagnosed a complicated urinary tract infection (UTI) associated with a CVF due to peritoneal dissemination and started empirical treatment with sulbactam/ampicillin. Given the absence of active inflammatory findings around the fistula on MRI and the patient's physical frailty, we decided to place a covered SEMS to close the fistula. Under fluoroscopic and endoscopic guidance, a covered colonic SEMS of 80-mm length and 20-mm diameter was successfully deployed, and the fistula was sealed immediately after placement. Urine culture on day 3 after stenting was negative for bacteria, and a contrast study on day 5 showed no fistula. The patient was discharged home on day 6 with no complications. The UTI did not recur for 4 months after discharge.
A covered colonic SEMS was useful for sealing a malignant CVF in a patient unfit for surgery, and MRI was valuable to determine the status of the fistula. A covered colonic SEMS could be an alternative to surgical treatment for CVFs in patients who require palliative care.
结肠膀胱瘘(CVF)通常通过切除含有瘘管的肠段或建立去功能化造口来治疗。我们在此报告一例通过放置覆膜结肠自膨式金属支架(SEMS)成功闭合瘘管并避免结肠造口术的病例,该病例为一名患有恶性CVF的患者的姑息治疗。
一名75岁男性因直肠癌复发性腹膜播散正在接受氟尿嘧啶和伊立替康静脉输注化疗加贝伐单抗治疗,因发热伴血尿入住我院。血液检查显示中度炎症反应(白细胞计数,9200/mm;C反应蛋白,11.03mg/dL;降钙素原,1.33ng/mL)。尿沉渣检查显示严重菌尿。腹部增强CT显示膀胱内气体、膀胱后壁增厚以及与膀胱后壁相邻的乙状结肠壁不规则增厚。磁共振成像(MRI)清楚地显示膀胱与乙状结肠之间存在瘘管。结肠镜检查发现距肛门边缘15cm处有环形恶性狭窄,通过水溶性造影剂确定存在膀胱瘘。我们诊断为因腹膜播散导致的与CVF相关的复杂性尿路感染(UTI),并开始使用舒巴坦/氨苄西林进行经验性治疗。鉴于MRI显示瘘管周围无活动性炎症表现且患者身体虚弱,我们决定放置覆膜SEMS以闭合瘘管。在荧光镜和内镜引导下,成功置入了一根长度为80mm、直径为20mm的覆膜结肠SEMS,置入后瘘管立即封闭。置入支架后第3天的尿培养细菌呈阴性,第5天的造影检查显示无瘘管。患者于第6天出院,无并发症。出院后4个月UTI未复发。
覆膜结肠SEMS对于不适合手术的患者闭合恶性CVF有用,MRI对于确定瘘管状态有价值。覆膜结肠SEMS对于需要姑息治疗的CVF患者可能是手术治疗的替代方法。