Faculty of Health and Social Development, University of British Columbia - Okanagan Campus, Kelowna, British Columbia, Canada.
Institute for Positive Psychology & Education, Australian Catholic University, Melbourne, Victoria, Australia.
Int J Behav Nutr Phys Act. 2023 Nov 21;20(1):134. doi: 10.1186/s12966-023-01535-w.
To determine rates of compliance (i.e., supervised intervention attendance) and adherence (i.e., unsupervised physical activity completion) to high-intensity interval training (HIIT) among insufficiently active adults and adults with a medical condition, and determine whether compliance and adherence rates were different between HIIT and moderate-intensity continuous training (MICT).
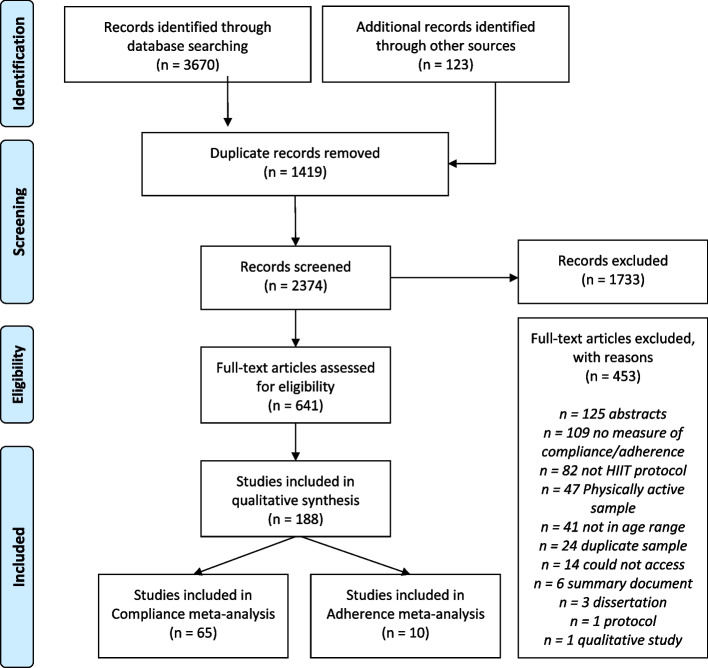
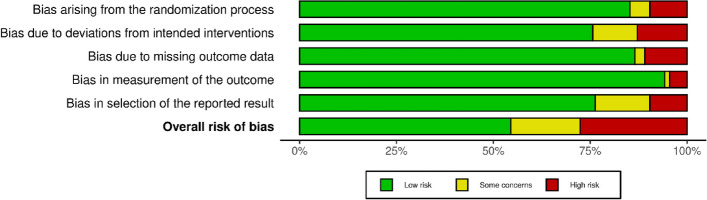
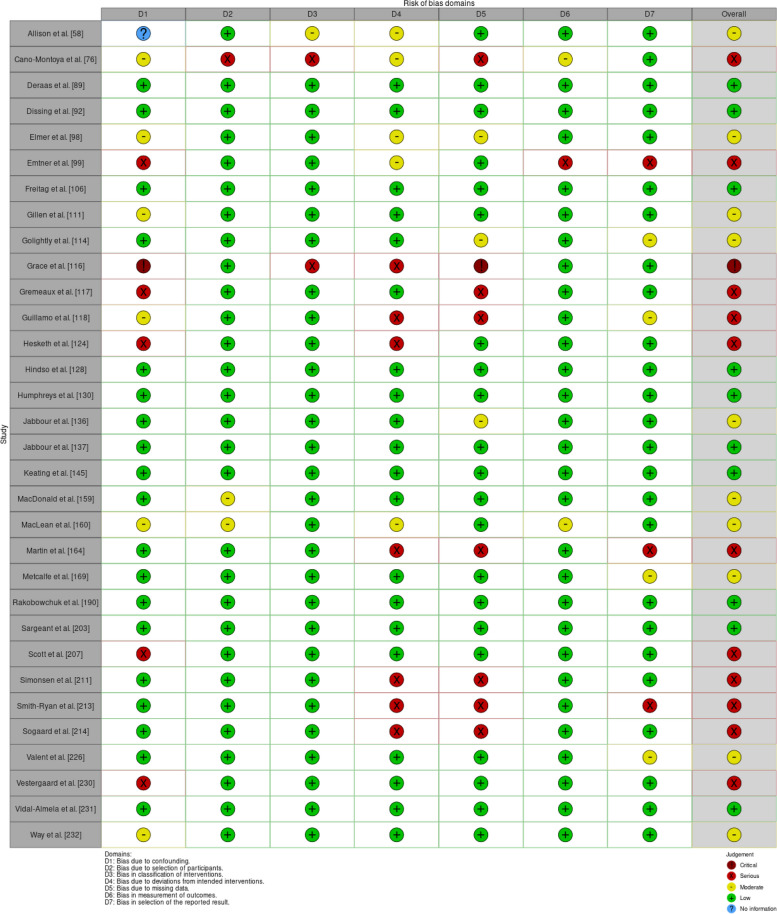
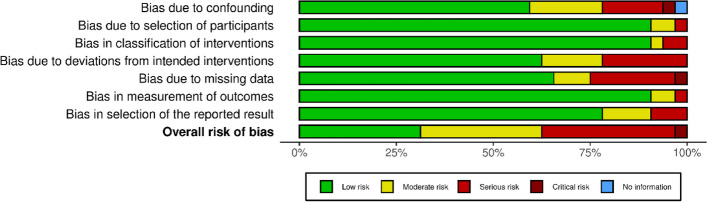
Articles on adults in a HIIT intervention and who were either insufficiently active or had a medical condition were included. MEDLINE, EMBASE, PsychINFO, SPORTDiscus, CINAHL, and Web of Science were searched. Article screening and data extraction were completed by two independent reviewers. Risk of bias was assessed using RoB 2.0 or ROBINS-I. Meta-analyses were conducted to discern differences in compliance and adherence between HIIT vs. MICT. Sensitivity analyses, publication bias, sub-group analyses, and quality appraisal were conducted for each meta-analysis.
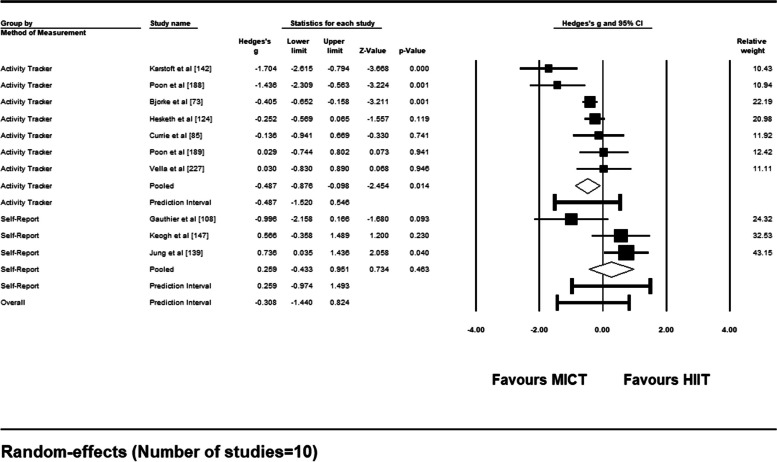
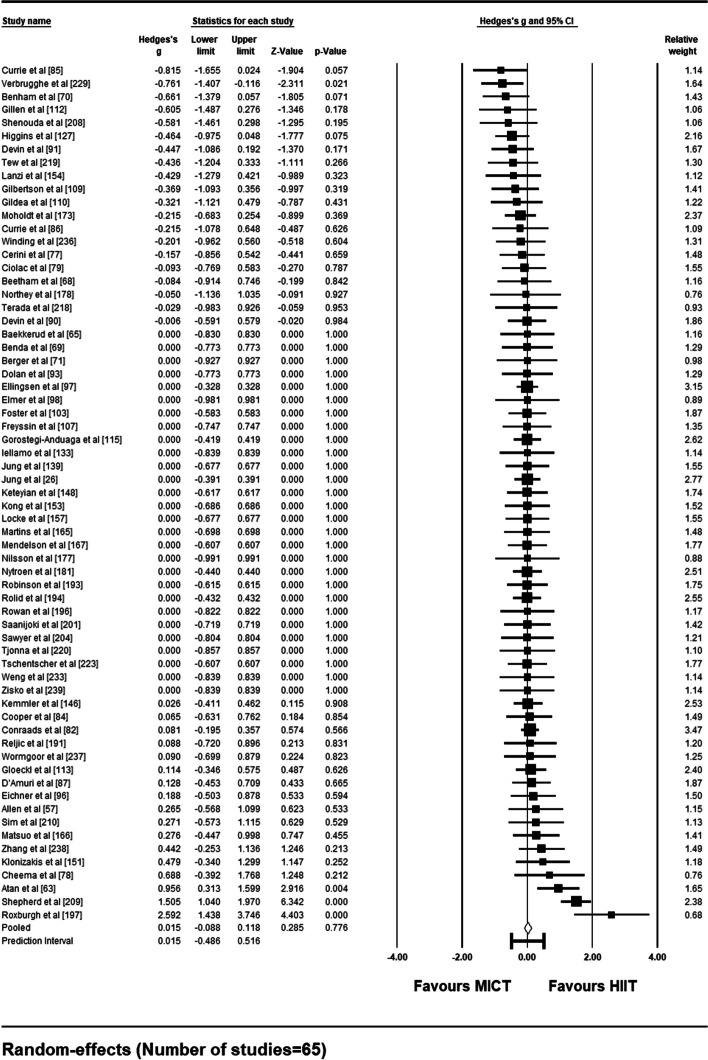
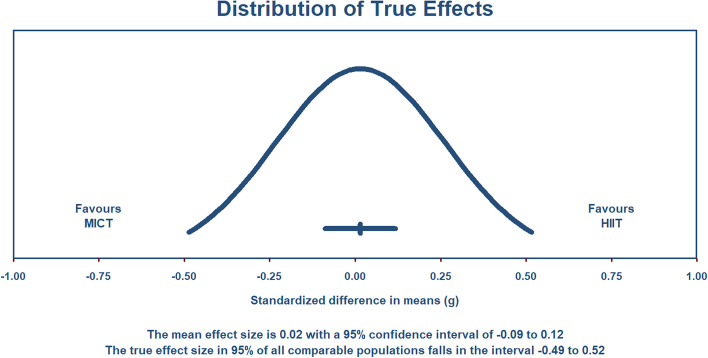
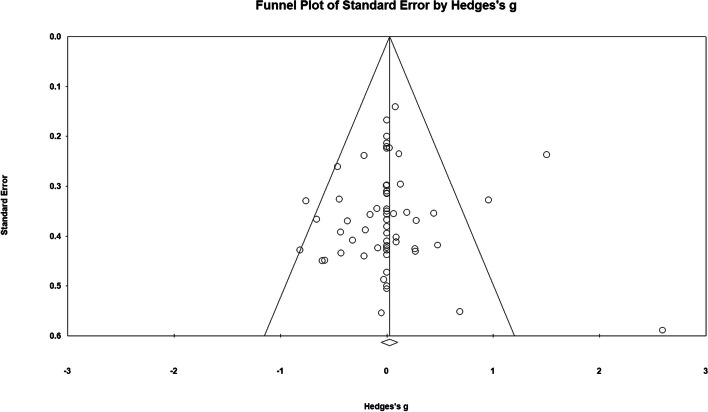
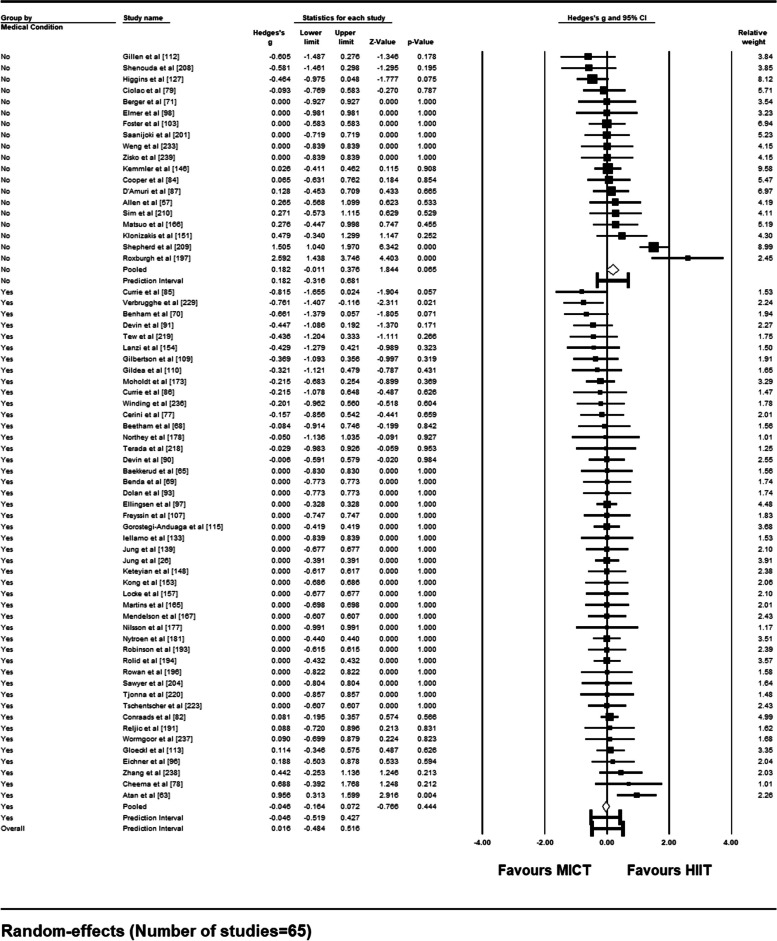
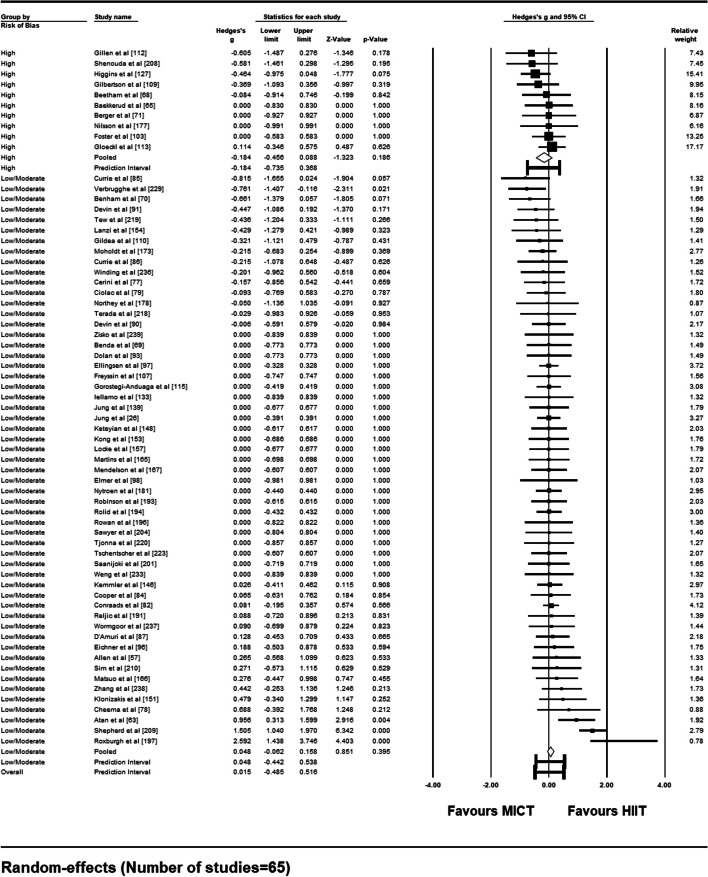
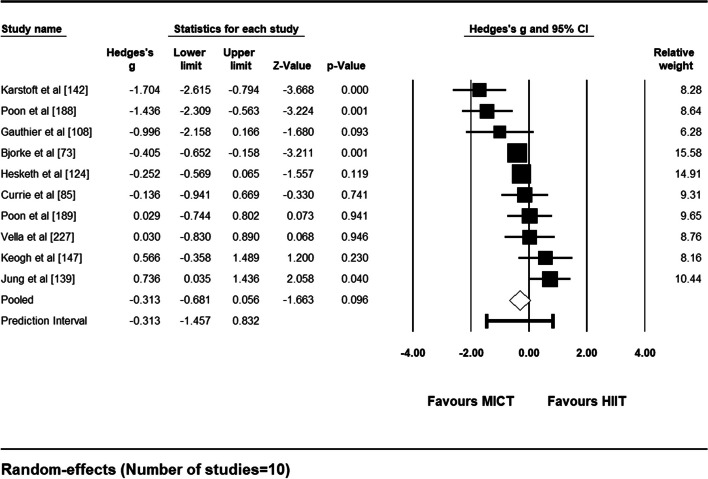
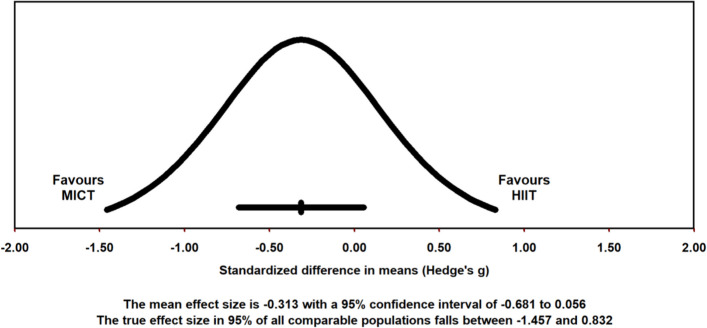
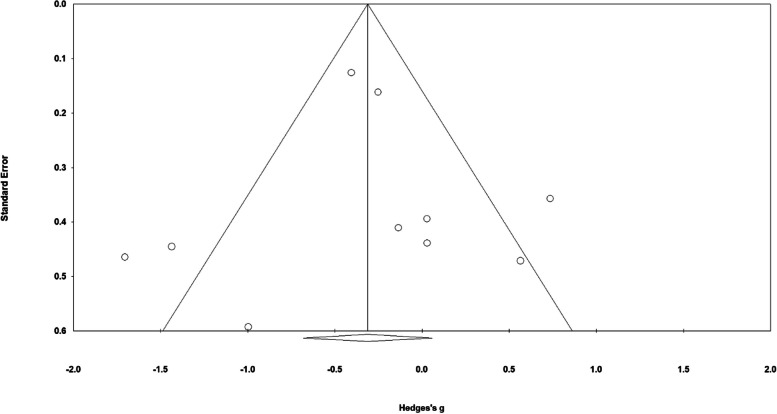
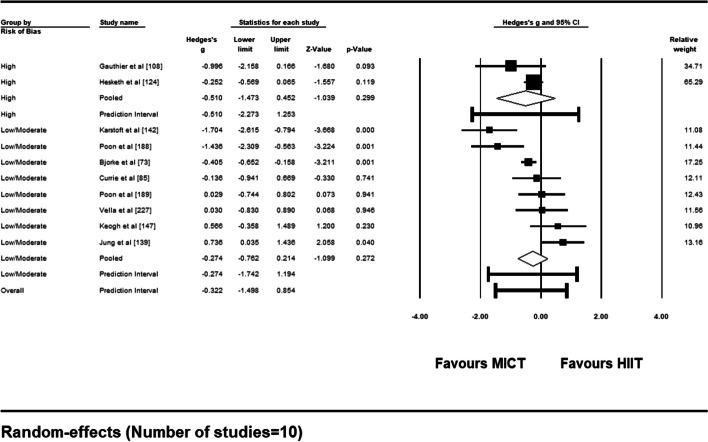
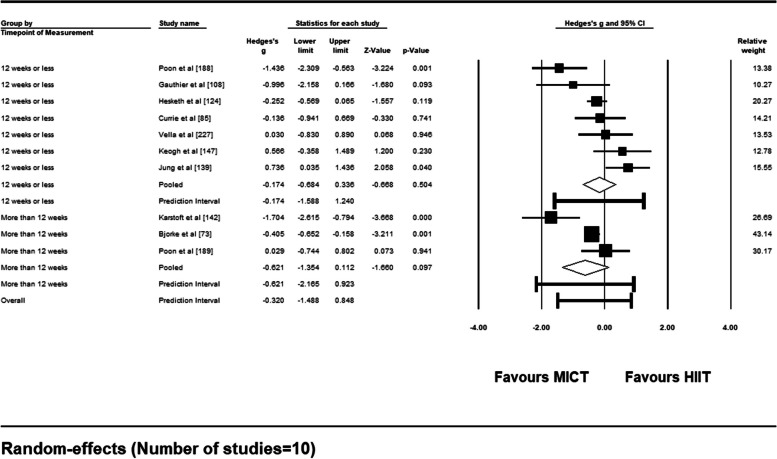
One hundred eighty-eight unique studies were included (n = 8928 participants). Compliance to HIIT interventions averaged 89.4% (SD:11.8%), while adherence to HIIT averaged 63% (SD: 21.1%). Compliance and adherence to MICT averaged 92.5% (SD:10.6%) and 68.2% (SD:16.2%), respectively. Based on 65 studies included in the meta-analysis, compliance rates were not different between supervised HIIT and MICT interventions [Hedge's g = 0.015 (95%CI: - 0.088-0.118), p = .78]. Results were robust and low risk of publication bias was detected. No differences were detected based on sub-group analyses comparing medical conditions or risk of bias of studies. Quality of the evidence was rated as moderate over concerns in the directness of the evidence. Based on 10 studies, adherence rates were not different between unsupervised HIIT and MICT interventions [Hedge's g = - 0.313 (95%CI: - 0.681-0.056), p = .096]. Sub-group analysis points to differences in adherence rates dependent on the method of outcome measurement. Adherence results should be interpreted with caution due to very low quality of evidence.
Compliance to HIIT and MICT was high among insufficiently active adults and adults with a medical condition. Adherence to HIIT and MICT was relatively moderate, although there was high heterogeneity and very low quality of evidence. Further research should take into consideration exercise protocols employed, methods of outcome measurement, and measurement timepoints.
This review was registered in the PROSPERO database and given the identifier CRD42019103313.
为了确定低强度活动成年人和有医疗条件的成年人对高强度间歇训练(HIIT)的依从性(即监督干预参与)和坚持性(即非监督体力活动完成)的比率,并确定 HIIT 和中等强度持续训练(MICT)之间的依从性和坚持率是否存在差异。
纳入了对 HIIT 干预中低强度活动或有医疗条件的成年人进行的研究。检索了 MEDLINE、EMBASE、PsychINFO、SPORTDiscus、CINAHL 和 Web of Science。由两名独立评审员进行文章筛选和数据提取。使用 RoB 2.0 或 ROBINS-I 评估偏倚风险。进行荟萃分析以辨别 HIIT 与 MICT 之间的依从性和坚持率差异。对每项荟萃分析进行敏感性分析、发表偏倚、亚组分析和质量评估。
共纳入 188 项独特的研究(n=8928 名参与者)。HIIT 干预的依从率平均为 89.4%(SD:11.8%),而 HIIT 的坚持率平均为 63%(SD:21.1%)。MICT 的依从率和坚持率平均为 92.5%(SD:10.6%)和 68.2%(SD:16.2%)。基于纳入的 65 项荟萃分析研究,监督 HIIT 和 MICT 干预的依从率没有差异[Hedge's g=0.015(95%CI:-0.088-0.118),p=0.78]。结果稳健,且发表偏倚风险低。基于比较医疗条件或研究偏倚风险的亚组分析,未发现差异。对证据直接性的关注,证据质量评为中度。基于 10 项研究,无监督 HIIT 和 MICT 干预的坚持率没有差异[Hedge's g=-0.313(95%CI:-0.681-0.056),p=0.096]。亚组分析表明,由于证据质量极低,坚持率取决于结局测量方法。由于证据质量极低,应谨慎解释坚持率结果。
低强度活动成年人和有医疗条件的成年人对 HIIT 和 MICT 的依从性较高。HIIT 和 MICT 的坚持率相对适中,尽管存在高度异质性和极低的证据质量。进一步的研究应考虑所采用的运动方案、结局测量方法和测量时间点。
本综述在 PROSPERO 数据库中进行了登记,并获得了 CRD42019103313 标识符。