Metabolic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, MD.
Department of Epidemiology, The University of Texas MD Anderson Cancer Center, Houston, TX.
Ann Epidemiol. 2023 Dec;88:15-22. doi: 10.1016/j.annepidem.2023.10.008. Epub 2023 Oct 29.
Inflammatory bowel disease (IBD) has a rising global prevalence. However, the understanding of its impact on mortality remains inconsistent so we explored the association between IBD and all-cause and cause-specific mortality.
This study included 502,369 participants from the UK Biobank, a large, population-based, prospective cohort study with mortality data through 2022. IBD was defined by baseline self-report or from primary care or hospital admission data. We estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for all-cause and cause-specific mortality in multivariable Cox proportional hazards regression models.
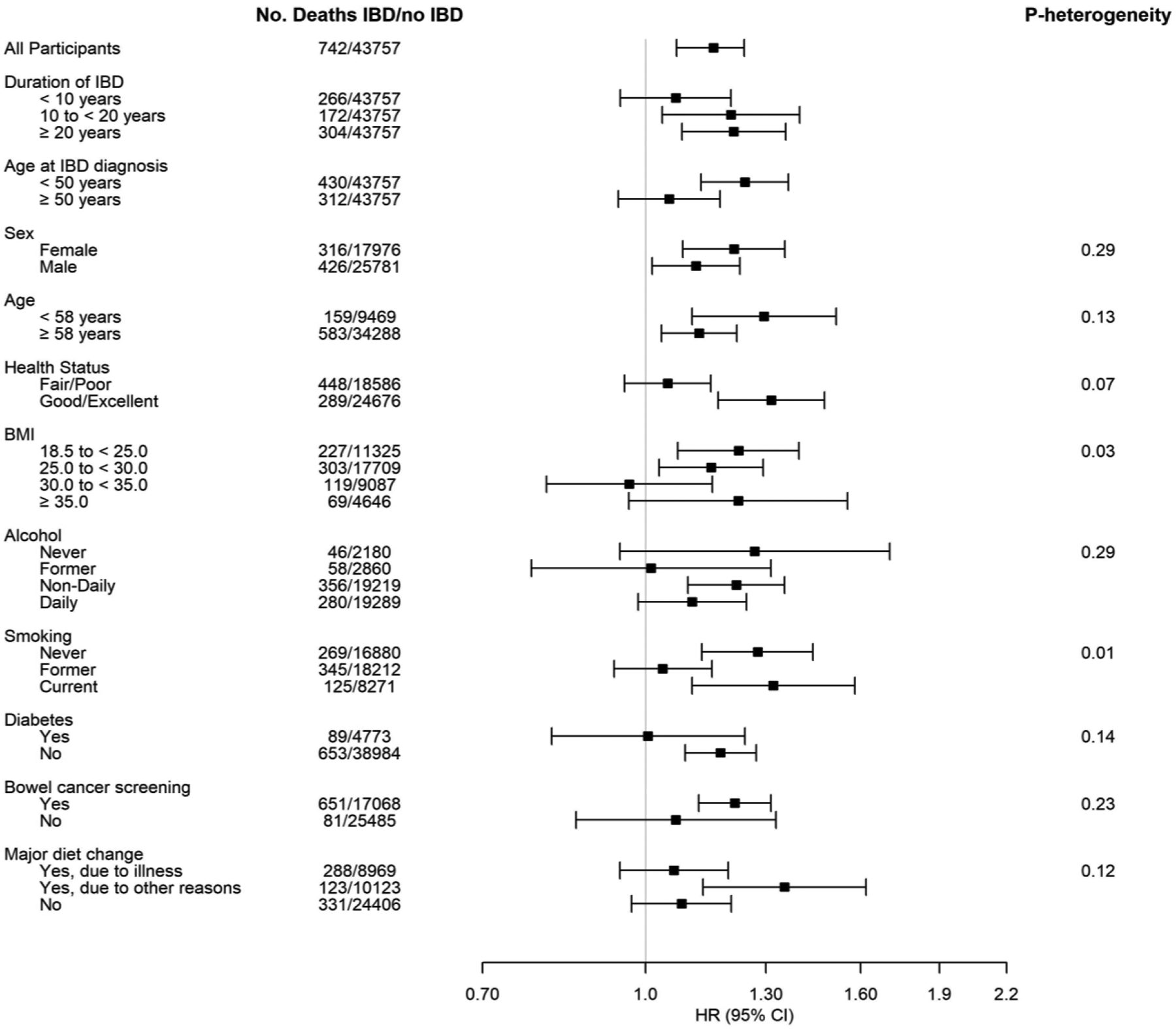
A total of 5799 (1.2%) participants had a history of IBD at baseline. After a median follow-up of 13.7 years, 44,499 deaths occurred. Having IBD was associated with an increased risk of death from all causes (HR = 1.16, 95% CI = 1.07-1.24) and cancer (HR = 1.16, 95% CI = 1.05-1.30), particularly colorectal cancer (CRC) (HR = 1.56, 95% CI = 1.17-2.09). We observed elevated breast cancer mortality rates for individuals with Crohn's disease, and increased CRC mortality rates for individuals with ulcerative colitis. In stratified analyses of IBD and all-cause mortality, mortality risk differed by individuals' duration of IBD, age at IBD diagnosis, body mass index (BMI) (P = 0.03) and smoking status (P = 0.01). Positive associations between IBD and all-cause mortality were detected in individuals diagnosed with IBD for 10 years or longer, those diagnosed before the age of 50, all BMI subgroups except obese individuals, and in never or current, but not former smokers.
We found that having IBD was associated with increased risks of mortality from all causes, all cancers, and CRC. This underscores the importance of enhanced patient management strategies and targeted prevention efforts in individuals with IBD.
炎症性肠病(IBD)在全球的发病率呈上升趋势。然而,人们对其死亡率的影响仍存在不一致的认识,因此我们探讨了 IBD 与全因和特定原因死亡率之间的关系。
本研究纳入了来自英国生物银行的 502369 名参与者,这是一项大型的、基于人群的前瞻性队列研究,通过 2022 年的数据来评估死亡率。IBD 通过基线自我报告或初级保健或住院数据来定义。我们使用多变量 Cox 比例风险回归模型来估计全因和特定原因死亡率的风险比(HR)和 95%置信区间(CI)。
共有 5799 名(1.2%)参与者在基线时有 IBD 病史。在中位随访 13.7 年后,共发生了 44499 例死亡。患有 IBD 与全因死亡风险增加相关(HR=1.16,95%CI=1.07-1.24)和癌症(HR=1.16,95%CI=1.05-1.30),尤其是结直肠癌(CRC)(HR=1.56,95%CI=1.17-2.09)。我们观察到患有克罗恩病的个体乳腺癌死亡率升高,而患有溃疡性结肠炎的个体 CRC 死亡率升高。在 IBD 和全因死亡率的分层分析中,死亡率风险因个体 IBD 的持续时间、IBD 诊断时的年龄、体重指数(BMI)(P=0.03)和吸烟状况(P=0.01)而异。在患有 IBD 10 年或以上、50 岁以下诊断、除肥胖者以外的所有 BMI 亚组以及从不吸烟或当前吸烟但非既往吸烟者中,均检测到 IBD 与全因死亡率之间的正相关关系。
我们发现患有 IBD 与全因死亡率、所有癌症死亡率和 CRC 死亡率升高相关。这突显了在 IBD 患者中加强患者管理策略和有针对性的预防措施的重要性。