Cawley Paul, Padormo Francesco, Cromb Daniel, Almalbis Jennifer, Marenzana Massimo, Teixeira Rui, Uus Alena, O'Muircheartaigh Jonathan, Williams Steven C R, Counsell Serena J, Arichi Tomoki, Rutherford Mary A, Hajnal Joseph V, Edwards A David
Centre for the Developing Brain, School of Biomedical Engineering and Imaging Sciences, King's College London, London SE1 7EH, UK.
Neonatal Intensive Care Unit, Evelina Children's Hospital London, St Thomas' Hospital, 6th Floor North Wing, Westminster Bridge Road, London SE1 7EH, UK.
EClinicalMedicine. 2023 Oct 10;65:102253. doi: 10.1016/j.eclinm.2023.102253. eCollection 2023 Nov.
Magnetic Resonance (MR) imaging is key for investigation of suspected newborn brain abnormalities. Access is limited in low-resource settings and challenging in infants needing intensive care. Portable ultralow field (ULF) MRI is showing promise in bedside adult brain imaging. Use in infants and children has been limited as brain-tissue composition differences necessitate sequence modification. The aim of this study was to develop neonatal-specific ULF structural sequences and test these across a range of gestational maturities and pathologies to inform future validation studies.
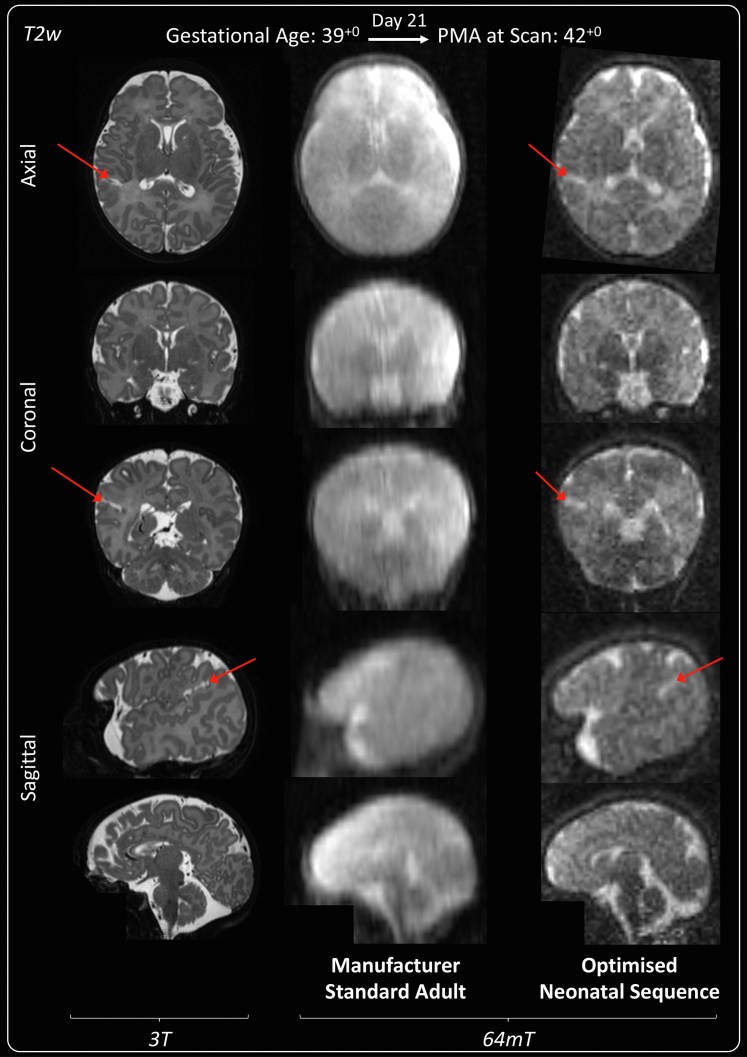
Prospective cohort study within a UK neonatal specialist referral centre. Infants undergoing 3T MRI were recruited for paired ULF (64mT) portable MRI by convenience sampling from the neonatal unit and post-natal ward. Key inclusion criteria: 1) Infants with risk or suspicion of brain abnormality, or 2) preterm and term infants without suspicion of major genetic, chromosomal or neurological abnormality. Exclusions: presence of contra-indication for MR scanning. ULF sequence parameters were optimised for neonatal brain-tissues by iterative and explorative design. Neuroanatomic and pathologic features were compared by unblinded review, informing optimisation of subsequent sequence generations in a step-wise manner. Main outcome: visual identification of healthy and abnormal brain tissues/structures. ULF MR spectroscopy, diffusion, susceptibility weighted imaging, arteriography, and venography require pre-clinical technical development and have not been tested.
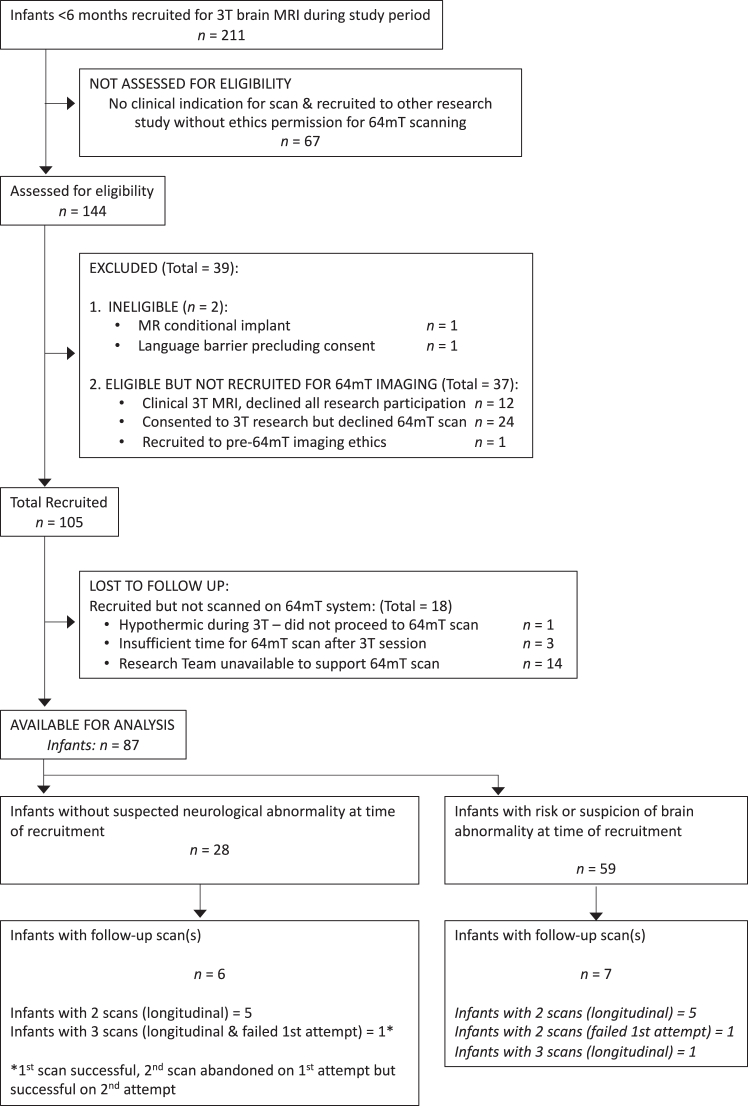
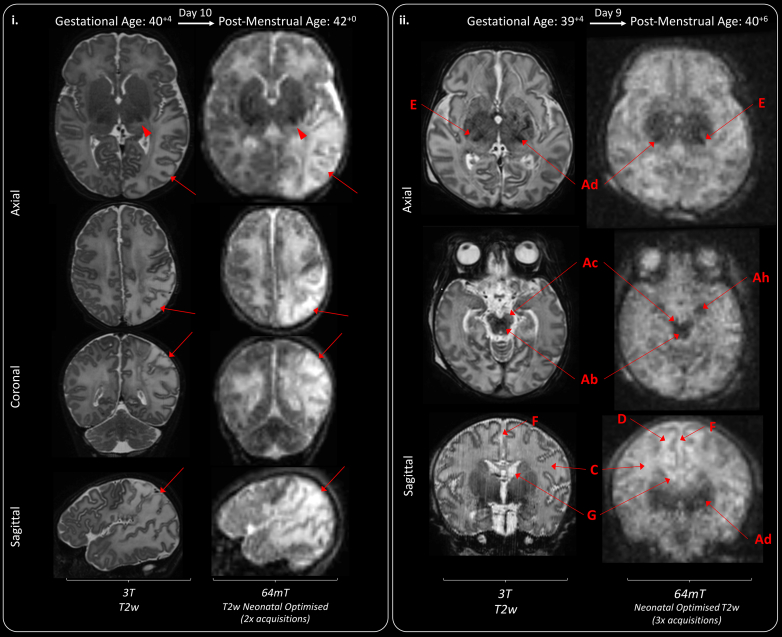
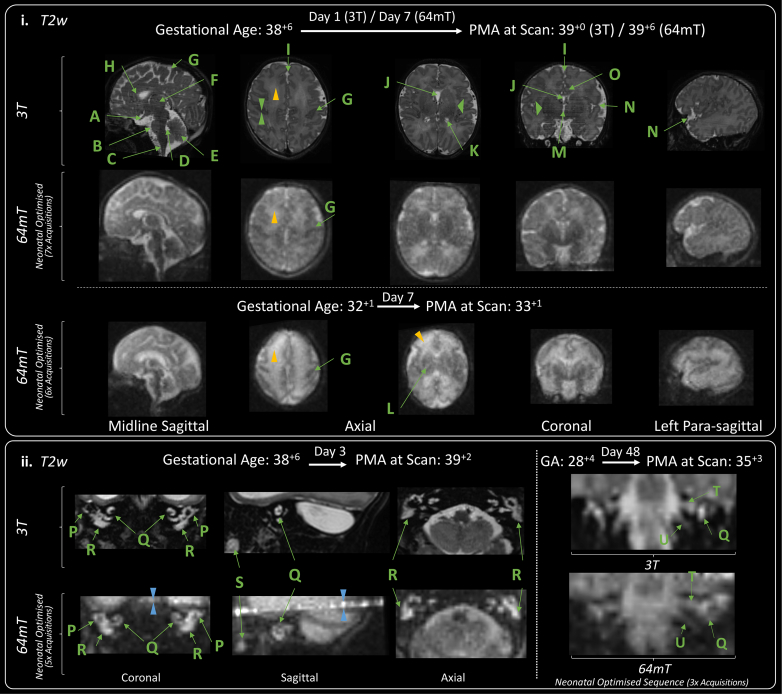
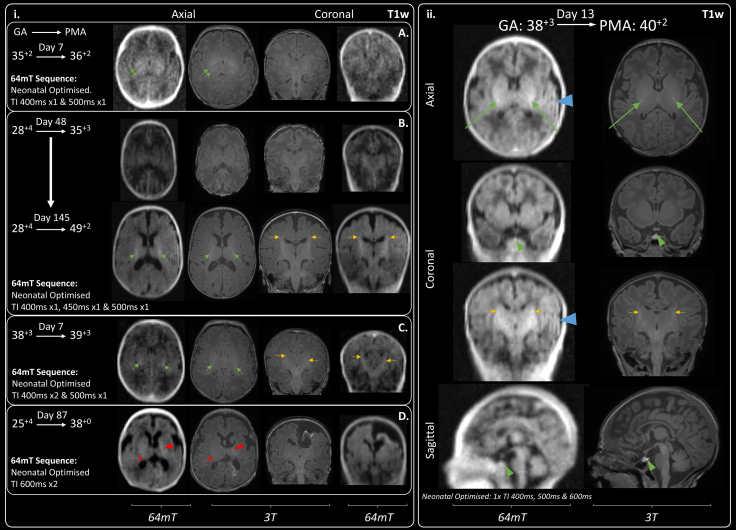
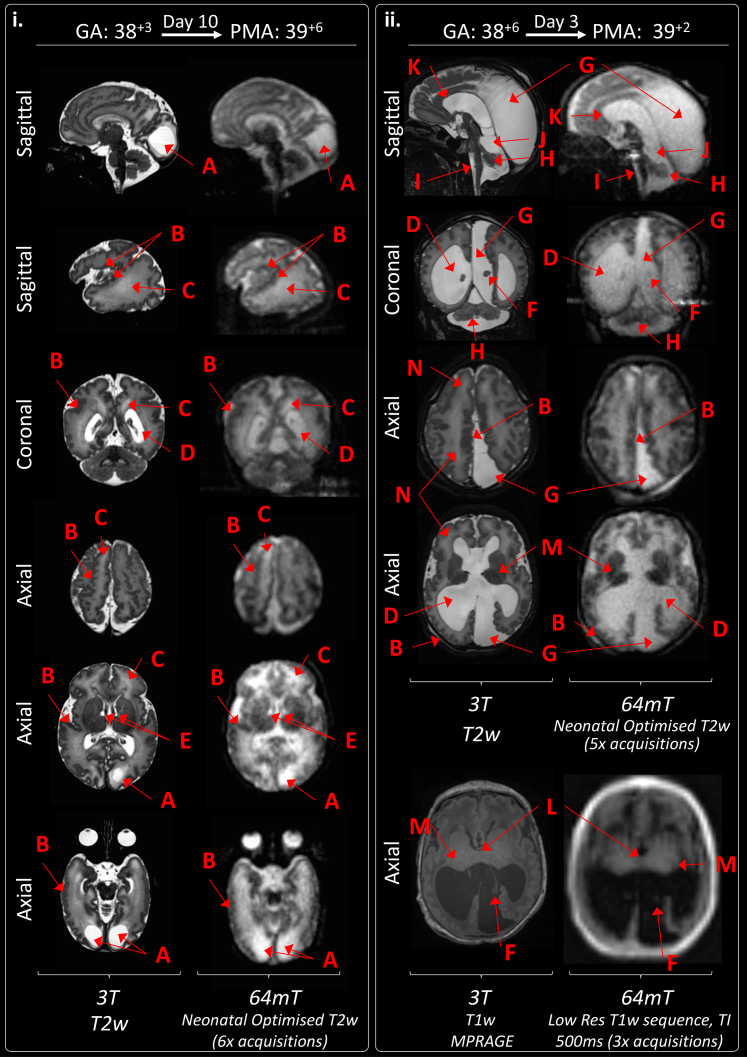
Between September 23, 2021 and October 25, 2022, 102 paired scans were acquired in 87 infants; 1.17 paired scans per infant. Median age 9 days, median postmenstrual age 40 weeks (range: 31-53). Infants had a range of intensive care requirements. No adverse events observed. Optimised ULF sequences can visualise key neuroanatomy and brain abnormalities. In finalised neonatal sequences: T2w imaging distinguished grey and white matter (7/7 infants), ventricles (7/7), pituitary tissue (5/7), corpus callosum (7/7) and optic nerves (7/7). Signal congruence was seen within the posterior limb of the internal capsule in 10/11 infants on finalised T1w scans. In addition, brain abnormalities visualised on ULF optimised sequences have similar MR signal patterns to 3T imaging, including injury secondary to infarction (6/6 infants on T2w scans), hypoxia-ischaemia (abnormal signal in basal ganglia, thalami and white matter 2/2 infants on T2w scans, cortical highlighting 1/1 infant on T1w scan), and congenital malformations: polymicrogyria 3/3, absent corpus callosum 2/2, and vermian hypoplasia 3/3 infants on T2w scans. Sequences are susceptible to motion corruption, noise, and ULF artefact. Non-identified pathologies were small or subtle.
On unblinded review, optimised portable MR can provide sufficient contrast, signal, and resolution for neuroanatomical identification and detection of a range of clinically important abnormalities. Blinded validation studies are now warranted.
The Bill and Melinda Gates Foundation, the MRC, the Wellcome/EPSRC Centre for Medical Engineering, the MRC Centre for Neurodevelopmental Disorders, and the National Institute for Health Research (NIHR) Biomedical Research Centres based at Guy's and St Thomas' and South London & Maudsley NHS Foundation Trusts and King's College London.
磁共振(MR)成像对于新生儿脑异常的诊断至关重要。在资源匮乏地区,设备的可及性有限,而对于需要重症监护的婴儿来说,进行磁共振成像检查颇具挑战。便携式超低场(ULF)磁共振成像在成人床边脑成像中展现出了应用前景。由于婴幼儿脑组织成分存在差异,需要对序列进行调整,因此其在婴幼儿中的应用受到限制。本研究旨在开发针对新生儿的ULF结构序列,并在不同孕周和病理情况下进行测试,为未来的验证研究提供依据。
在英国一家新生儿专科转诊中心开展前瞻性队列研究。通过便利抽样,从新生儿病房和产后病房招募接受3T磁共振成像检查的婴儿,进行配对的ULF(64mT)便携式磁共振成像检查。主要纳入标准:1)有脑异常风险或疑似脑异常的婴儿;2)无重大遗传、染色体或神经异常的早产和足月婴儿。排除标准:存在磁共振扫描禁忌证。通过迭代和探索性设计,对ULF序列参数进行优化,以适应新生儿脑组织。通过非盲法评估比较神经解剖和病理特征,逐步为后续序列的优化提供依据。主要观察指标:通过视觉识别健康和异常的脑组织/结构。ULF磁共振波谱、扩散加权成像、磁敏感加权成像、动脉造影和静脉造影等技术尚需进行临床前技术开发,尚未进行测试。
2021年9月23日至2022年10月25日期间,对87名婴儿进行了102次配对扫描,每名婴儿平均进行1.17次配对扫描。中位年龄为9天,中位孕龄为40周(范围:31 - 53周)。婴儿有一系列重症监护需求。未观察到不良事件。优化后的ULF序列能够清晰显示关键神经解剖结构和脑异常。在最终确定的新生儿序列中:T2加权成像能够区分灰质和白质(7/7名婴儿)、脑室(7/7)、垂体组织(5/7)、胼胝体(7/7)和视神经(7/7)。在最终确定的T1加权扫描中,10/11名婴儿的内囊后肢信号一致。此外,在ULF优化序列上显示的脑异常与3T成像具有相似的磁共振信号模式,包括梗死继发损伤(T2加权扫描中6/6名婴儿)、缺氧缺血(T2加权扫描中2/2名婴儿基底节、丘脑和白质出现异常信号,T1加权扫描中1/1名婴儿皮质出现高亮信号)以及先天性畸形:多小脑回3/3名婴儿、胼胝体缺如2/2名婴儿、小脑蚓部发育不全3/3名婴儿(T2加权扫描)。序列容易受到运动干扰、噪声和ULF伪影的影响。未识别出的病变较小或较为隐匿。
通过非盲法评估,优化后的便携式磁共振成像能够提供足够的对比度、信号和分辨率,用于神经解剖结构的识别以及一系列临床重要异常的检测。现在有必要进行盲法验证研究。
比尔及梅琳达·盖茨基金会、医学研究理事会、惠康/工程和物理科学研究理事会医学工程中心、医学研究理事会神经发育障碍中心以及基于盖伊和圣托马斯医院以及南伦敦和莫兹利国民保健服务基金会信托基金和伦敦国王学院的国家卫生研究院(NIHR)生物医学研究中心。