Department of Psychiatry, University of Toronto, Toronto, ON, M5T 1R8, Canada.
Department of Psychiatry, Women's College Hospital and Research Institute, 76 Grenville Street, Toronto, ON, M5S 1B2, Canada.
BMC Psychiatry. 2023 Dec 18;23(1):950. doi: 10.1186/s12888-023-05444-x.
Mothers with a history of adverse childhood experiences (ACE) are at elevated risk for postpartum mental illness and impairment in the mother-infant relationship. Interventions attending to maternal-infant interactions may improve outcomes for these parents and their children, but barriers to accessing in-person postpartum care limit uptake. We adapted a postpartum psychotherapy group for mothers with mental illness (e.g., mood, anxiety, trauma-related disorders) and ACE for live video-based delivery, and evaluated feasibility, acceptability, and preliminary efficacy in an open-label pilot study.
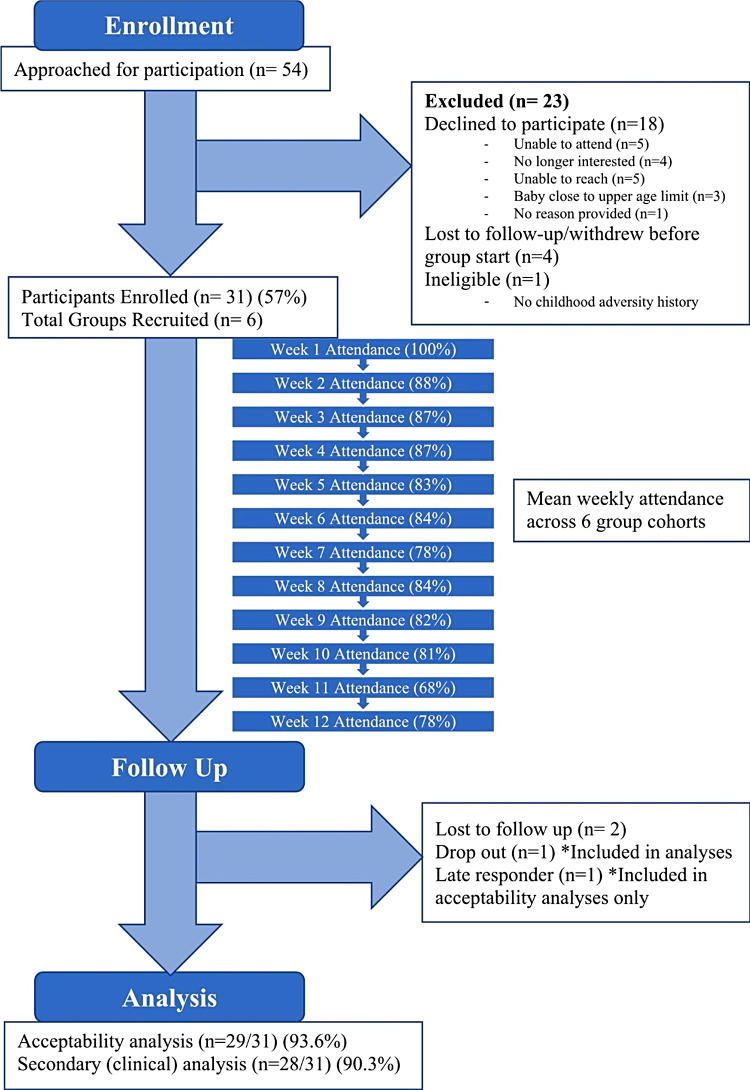
We recruited adults with children (6-18 months) from a perinatal psychiatry program in Toronto, Canada. The intervention was a live video-based 12-week interactive psychotherapy group focused on maternal symptoms and maternal-infant relationships. The primary outcome was feasibility, including feasibility of recruitment and retention, fidelity of the intervention, and acceptability to patients and group providers. Maternal clinical outcomes were compared pre- to post-intervention, as secondary outcomes.
We recruited 31 participants (mean age 36.5 years (SD 3.9)) into 6 groups; 93.6% (n = 29) completed post-group questionnaires, and n = 20 completed an optional post-group acceptability interview. Mean weekly group attendance was 83% (IQR 80-87); one participant (3.2%) dropped out. All group components were implemented as planned, except for dyadic exercises where facilitator observation of dyads was replaced with unobserved mother-infant exercises followed by in-group reflection. Participant acceptability was high (100% indicated the virtual group was easy to access, beneficial, and reduced barriers to care). Mean maternal depressive [Edinburgh Postnatal Depression Scale: 14.6 (SD 4.2) vs. 11.8 (SD 4.2), paired t, p = 0.005] and post-traumatic stress [Posttraumatic Stress Disorder Checklist for DSM-5: 35.5 (SD 19.0) vs. 27.1 (SD 16.7)], paired t, p = 0.01] symptoms were significantly lower post vs. pre-group. No differences were observed on mean measures of anxiety, emotion regulation or parenting stress.
Recruitment and retention met a priori feasibility criteria. There were significant pre- to post-group reductions in maternal depressive and post-traumatic symptoms, supporting proceeding to larger-scale implementation and evaluation of the intervention, with adaptation of dyadic exercises.
有不良童年经历(ACE)的母亲产后患精神疾病和母婴关系受损的风险较高。关注母婴互动的干预措施可能会改善这些父母及其子女的结局,但获得产后护理的障碍限制了干预措施的普及。我们将针对患有精神疾病(如情绪、焦虑、创伤相关障碍)和 ACE 的母亲的产后心理治疗小组改编为基于视频的现场交付,并在一项开放标签试点研究中评估其可行性、可接受性和初步疗效。
我们从加拿大多伦多的围产期精神病学项目中招募了有 6-18 个月大子女的成年人。该干预措施是一个基于现场视频的 12 周互动心理治疗小组,重点关注母亲的症状和母婴关系。主要结局是可行性,包括招募和保留的可行性、干预措施的忠实度以及患者和小组提供者的可接受性。将母婴临床结局作为次要结局,在干预前和干预后进行比较。
我们将 31 名参与者(平均年龄 36.5 岁(SD 3.9))分为 6 组;93.6%(n=29)完成了小组后调查问卷,n=20 完成了可选的小组后可接受性访谈。平均每周小组出勤率为 83%(IQR 80-87);1 名参与者(3.2%)退出。除了二元练习外,所有小组组成部分都按计划实施,在二元练习中,协调员观察二元组被替换为未观察到的母婴练习,然后在小组内进行反思。参与者的可接受性很高(100%的人表示虚拟小组易于访问,有益且减少了获得护理的障碍)。母亲抑郁的平均程度[爱丁堡产后抑郁量表:14.6(SD 4.2)与 11.8(SD 4.2),配对 t,p=0.005]和创伤后应激[创伤后应激障碍检查表 DSM-5:35.5(SD 19.0)与 27.1(SD 16.7)],配对 t,p=0.01]症状在小组后比小组前显著降低。焦虑、情绪调节或育儿压力的平均测量值无差异。
招募和保留符合事先确定的可行性标准。与小组前相比,母亲抑郁和创伤后症状有显著的小组后降低,支持对干预措施进行更大规模的实施和评估,并对二元练习进行调整。