Vega-Figueroa Karlene, Silva-Melendez Pilar, Figueroa-Gonzalez Rocio, Colom-Diaz Andrea, Gonzalez Karina
Obstetrics and Gynecology, Centro Medico Episcopal San Lucas, Ponce, PRI.
Obstetrics and Gynecology, Ponce Health Sciences University, Ponce, PRI.
Cureus. 2023 Nov 18;15(11):e49006. doi: 10.7759/cureus.49006. eCollection 2023 Nov.
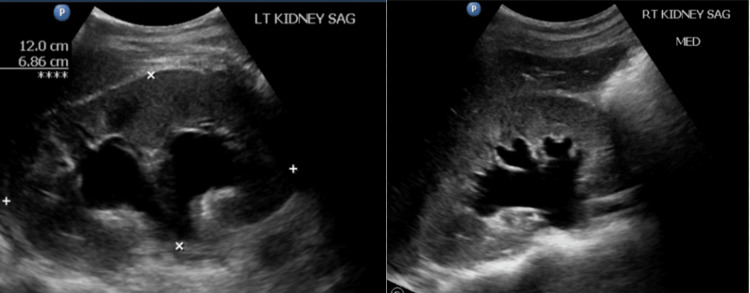
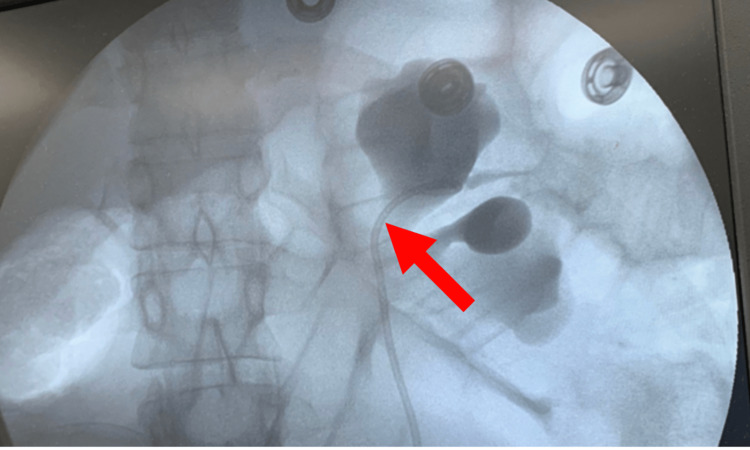
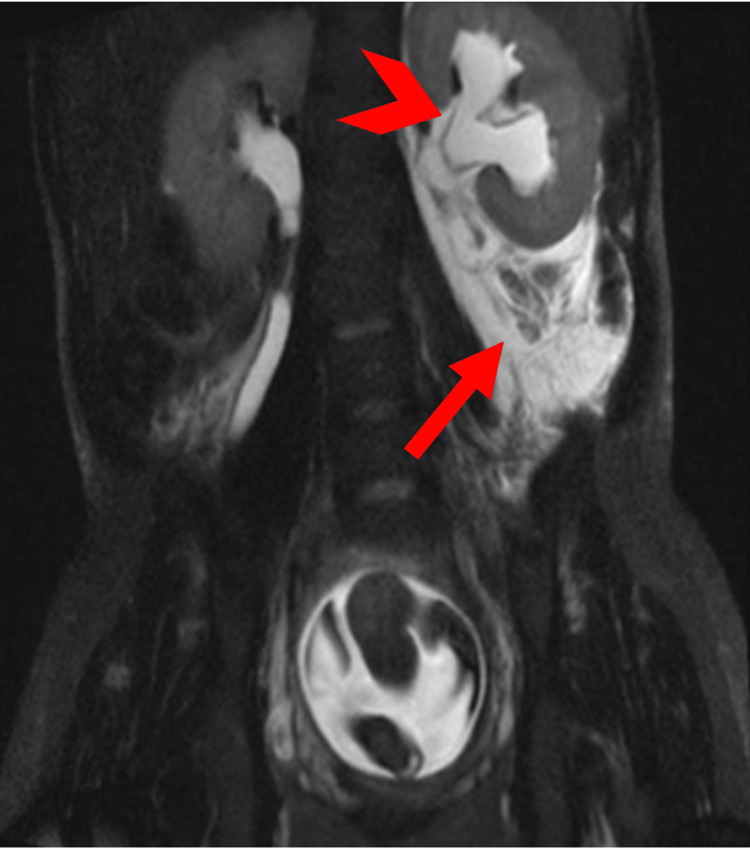
A spontaneous renal calyceal rupture in pregnancy is extremely rare and can be challenging to identify as its presentation can mimic other more common diagnoses, which can lead to a delay in management. Here, we describe an unusual case of renal calyceal rupture in a 24-year-old G2P0010 female with pregnancy at 26.5 weeks gestation age (WGA) who was admitted to the antepartum ward due to left flank pain and uterine contractions. A renal sonogram was performed, which revealed severe left hydronephrosis and the absence of the ipsilateral ureteral jet. Urinalysis was within normal limits, and her renal function was preserved. Laboratories were remarkable for elevated liver enzymes. Finally, an abdominopelvic MRI revealed the culprit, a calyceal rupture. Once the diagnosis was clear, a double J-stent was inserted using limited fluoroscopy with the goal of reducing intrarenal pressure and decreasing disease morbidity. The patient's symptoms significantly improved after double J-stent placement and resolved the following day. The patient further developed preeclampsia with severe features, which has previously been documented to occur in pregnant patients with renal tract ruptures. The diagnosis of a renal calyceal rupture in pregnancy is not straightforward, in part because of a lack of awareness of this pathology. Nevertheless, early identification can prevent unnecessary interventions and adverse outcomes. Its diagnosis can be made with MRI, and its management with ureteral stent placement shouldn't be delayed, and its association with preeclampsia should be further explored.
妊娠期自发性肾盏破裂极为罕见,且因其表现可能与其他更常见的诊断相似而难以识别,这可能导致治疗延迟。在此,我们描述一例不寻常的病例,一名24岁、孕2产0010、妊娠26.5周的女性因左侧腰痛和子宫收缩入住产前病房。进行了肾脏超声检查,结果显示左侧严重肾积水且同侧输尿管无喷射现象。尿液分析结果正常,肾功能得以保留。实验室检查显示肝酶升高。最后,腹部盆腔磁共振成像(MRI)发现了病因,即肾盏破裂。一旦诊断明确,在有限的荧光透视引导下插入双J支架,目的是降低肾内压力并降低疾病发病率。放置双J支架后患者症状明显改善,并于次日缓解。该患者进一步发展为伴有严重特征的先兆子痫,此前已有文献记载,这种情况在患有肾道破裂的孕妇中会发生。妊娠期肾盏破裂的诊断并不简单,部分原因是对这种病理情况缺乏认识。然而,早期识别可以避免不必要的干预和不良后果。其诊断可通过MRI做出,输尿管支架置入治疗不应延迟,且应进一步探讨其与先兆子痫的关联。