Research Program in Men's Health: Aging and Metabolism, Boston Claude D. Pepper Older Americans Independence Center, Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
Marcus Institute for Aging Research, Hebrew Senior Life, Division of Gerontology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, Massachusetts.
JAMA Netw Open. 2023 Dec 1;6(12):e2348692. doi: 10.1001/jamanetworkopen.2023.48692.
The effect of testosterone replacement therapy (TRT) on the risk of prostate cancer and other adverse prostate events is unknown.
To compare the effect of TRT vs placebo on the incidences of high-grade prostate cancers (Gleason score ≥4 + 3), any prostate cancer, acute urinary retention, invasive prostate procedures, and pharmacologic treatment for lower urinary tract symptoms in men with hypogonadism.
DESIGN, SETTING, AND PARTICIPANTS: This placebo-controlled, double-blind randomized clinical trial enrolled 5246 men (aged 45-80 years) from 316 US trial sites who had 2 testosterone concentrations less than 300 ng/dL, hypogonadal symptoms, and cardiovascular disease (CVD) or increased CVD risk. Men with prostate-specific antigen (PSA) concentrations greater than 3.0 ng/mL and International Prostate Symptom Score (IPSS) greater than 19 were excluded. Enrollment took place between May 23, 2018, and February 1, 2022, and end-of-study visits were conducted between May 31, 2022, and January 19, 2023.
Participants were randomized, with stratification for prior CVD, to topical 1.62% testosterone gel or placebo.
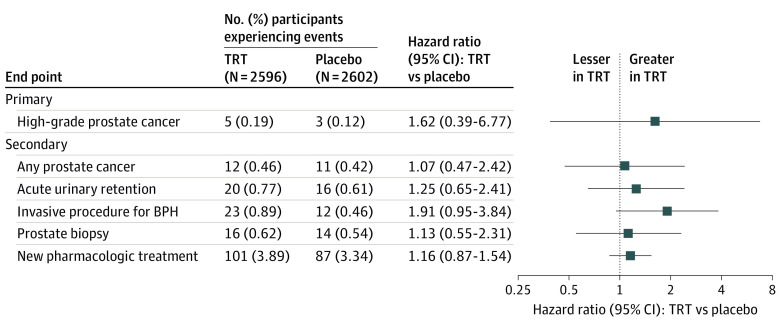
The primary prostate safety end point was the incidence of adjudicated high-grade prostate cancer. Secondary end points included incidence of any adjudicated prostate cancer, acute urinary retention, invasive prostate surgical procedure, prostate biopsy, and new pharmacologic treatment. Intervention effect was analyzed using a discrete-time proportional hazards model.
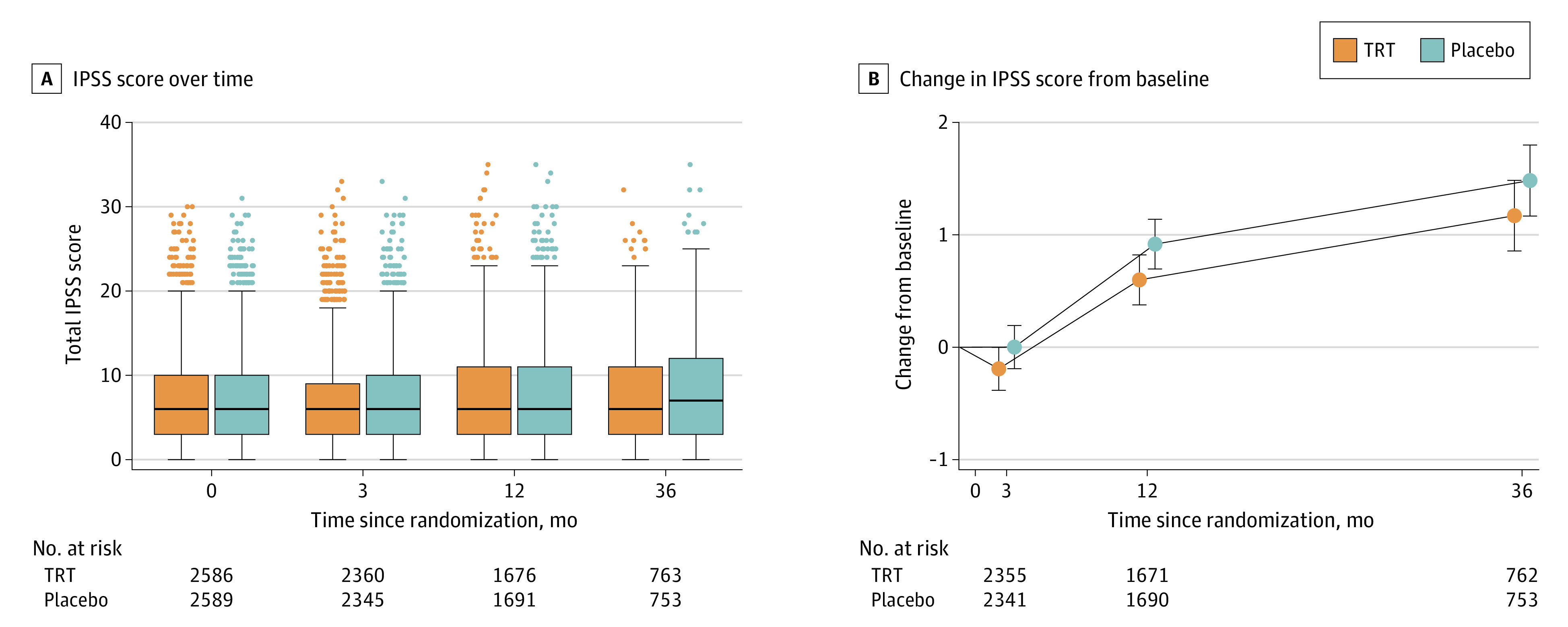
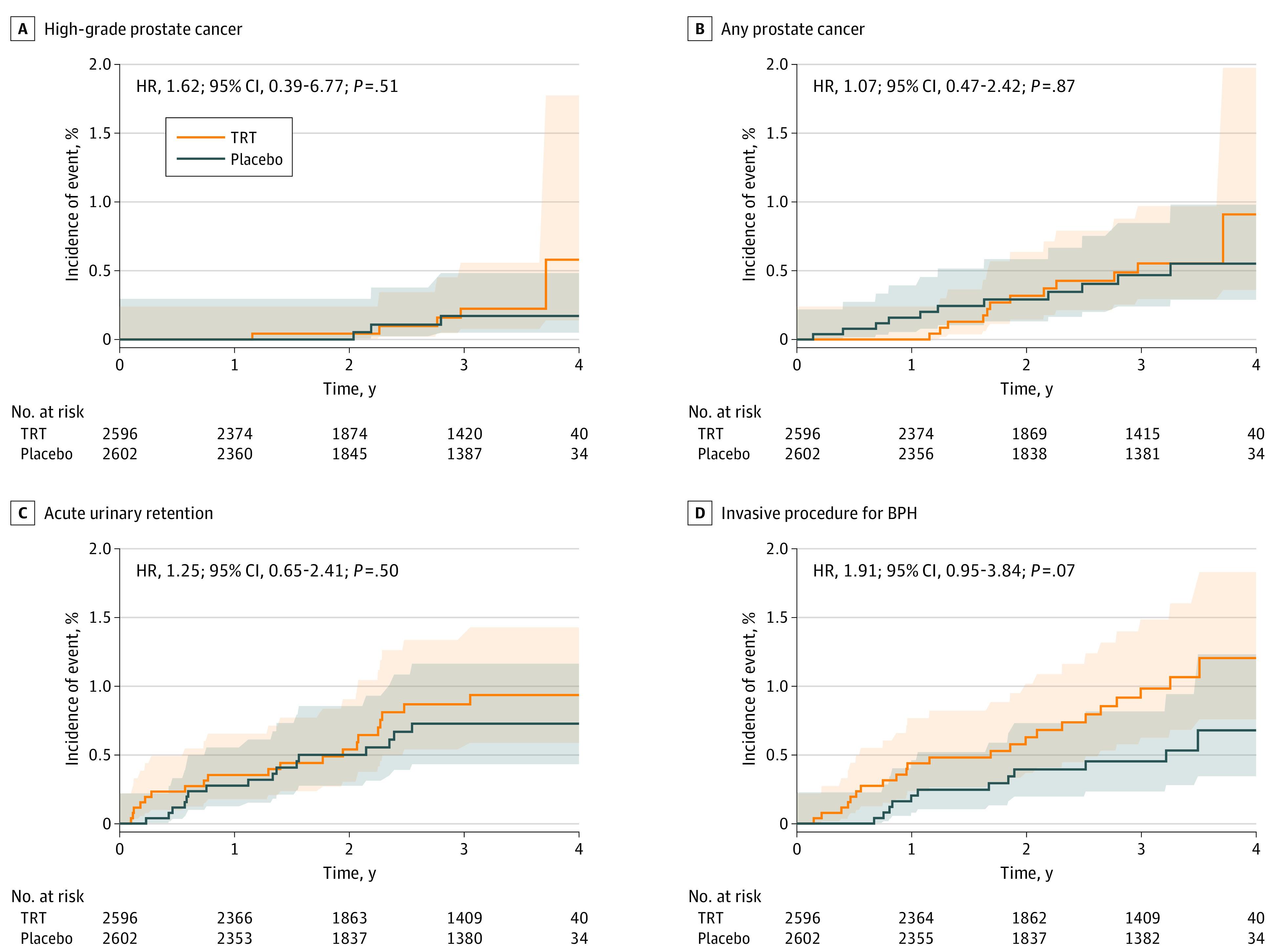
A total of 5204 men (mean [SD] age, 63.3 [7.9] years) were analyzed. At baseline, the mean (SD) PSA concentration was 0.92 (0.67) ng/mL, and the mean (SD) IPSS was 7.1 (5.6). The mean (SD) treatment duration as 21.8 (14.2) months in the TRT group and 21.6 (14.0) months in the placebo group. During 14 304 person-years of follow-up, the incidence of high-grade prostate cancer (5 of 2596 [0.19%] in the TRT group vs 3 of 2602 [0.12%] in the placebo group; hazard ratio, 1.62; 95% CI, 0.39-6.77; P = .51) did not differ significantly between groups; the incidences of any prostate cancer, acute urinary retention, invasive surgical procedures, prostate biopsy, and new pharmacologic treatment also did not differ significantly. Change in IPSS did not differ between groups. The PSA concentrations increased more in testosterone-treated than placebo-treated men.
In a population of middle-aged and older men with hypogonadism, carefully evaluated to exclude those at high risk of prostate cancer, the incidences of high-grade or any prostate cancer and other prostate events were low and did not differ significantly between testosterone- and placebo-treated men. The study's findings may facilitate a more informed appraisal of the potential risks of TRT.
ClinicalTrials.gov Identifier: NCT03518034.
睾丸激素替代疗法(TRT)对前列腺癌和其他前列腺不良事件的风险影响尚不清楚。
比较 TRT 与安慰剂对低促性腺激素血症男性的高级别前列腺癌(Gleason 评分≥4+3)、任何前列腺癌、急性尿潴留、前列腺侵袭性手术和下尿路症状药物治疗发生率的影响。
设计、地点和参与者:这是一项安慰剂对照、双盲随机临床试验,招募了 316 个美国试验点的 5246 名年龄在 45-80 岁之间的男性,他们有 2 种睾丸激素浓度低于 300ng/dL,有低促性腺激素症状和心血管疾病(CVD)或 CVD 风险增加。排除前列腺特异性抗原(PSA)浓度大于 3.0ng/mL 和国际前列腺症状评分(IPSS)大于 19 的男性。招募于 2018 年 5 月 23 日至 2022 年 2 月 1 日进行,研究结束时的随访于 2022 年 5 月 31 日至 2023 年 1 月 19 日进行。
参与者被随机分层,根据既往 CVD 情况,分为局部 1.62%睾酮凝胶或安慰剂。
主要前列腺安全性终点是经裁决的高级别前列腺癌的发生率。次要终点包括任何经裁决的前列腺癌、急性尿潴留、前列腺侵袭性手术、前列腺活检和新的药物治疗的发生率。干预效果使用离散时间比例风险模型进行分析。
共分析了 5204 名男性(平均[标准差]年龄,63.3[7.9]岁)。基线时,平均(标准差)PSA 浓度为 0.92(0.67)ng/mL,平均(标准差)IPSS 为 7.1(5.6)。TRT 组的平均(标准差)治疗持续时间为 21.8(14.2)个月,安慰剂组为 21.6(14.0)个月。在 14304 人年的随访中,高级别前列腺癌的发生率(TRT 组 5/2596[0.19%]与安慰剂组 3/2602[0.12%];危险比,1.62;95%CI,0.39-6.77;P=0.51)在两组间无显著差异;任何前列腺癌、急性尿潴留、侵袭性手术、前列腺活检和新的药物治疗的发生率也无显著差异。两组间 IPSS 变化无差异。与安慰剂组相比,接受睾丸激素治疗的男性 PSA 浓度升高更为明显。
在经过仔细评估排除了前列腺癌高危人群的中年和老年低促性腺激素血症男性中,高级别或任何前列腺癌和其他前列腺事件的发生率较低,且在睾丸激素和安慰剂治疗的男性中无显著差异。该研究结果可能有助于更全面地评估 TRT 的潜在风险。
ClinicalTrials.gov 标识符:NCT03518034。