Drug Usage and Pharmacy Practice Group, Division of Pharmacy and Optometry, Faculty of Biology, Medicine and Health, Centre for Pharmacoepidemiology and Drug Safety, Manchester Academic Health Science Centre, School of Health Sciences, University of Manchester, Oxford Road, Manchester, M13 9PT, UK.
Department of Public Health Pharmacy and Management, School of Pharmacy, Sefako Makgatho Health Sciences University, Molotlegi Street, Pretoria, 0208, South Africa.
BMC Med. 2024 Jan 2;22(1):5. doi: 10.1186/s12916-023-03213-x.
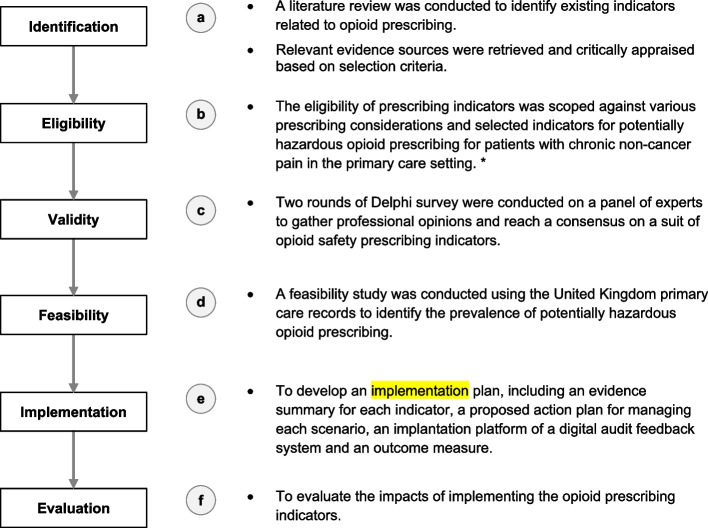
Long-term opioid use is associated with dependency, addiction, and serious adverse events. Although a framework to reduce inappropriate opioid prescribing exists, there is no consensus on prescribing indicators for preventable opioid-related problems in patients with chronic pain in primary care in the UK. This study aimed to identify opioid prescription scenarios for developing indicators for prescribing opioids to patients with chronic pain in primary care.
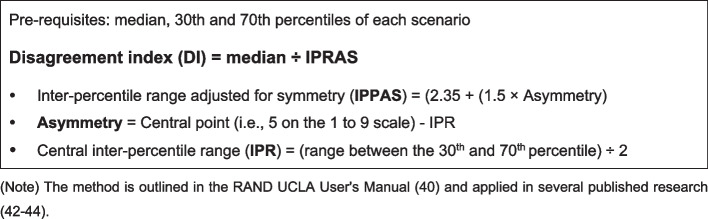
Scenarios of opioid prescribing indicators were identified from a literature review, guidelines, and government reports. Twenty-one indicators were identified and presented in various opioid scenarios concerning opioid-related harm and adverse effects, drug-drug interactions, and drug-disease interactions in certain disease conditions. After receiving ethics approval, two rounds of electronic Delphi panel technique surveys were conducted with 24 expert panellists from the UK (clinicians, pharmacists, and independent prescribers) from August 2020 to February 2021. Each indicator was rated on a 1-9 scale from inappropriate to appropriate. The score's median, 30th and 70th percentiles, and disagreement index were calculated.
The panel unanimously agreed that 15 out of the 21 opioid prescribing scenarios were inappropriate, primarily due to their potential for causing harm to patients. This consensus was reflected in the low appropriateness scores (median ranging from 1 to 3). There were no scenarios with a high consensus that prescribing was appropriate. The indicators were considered inappropriate due to drug-disease interactions (n = 8), drug-drug interactions (n = 2), adverse effects (n = 3), and prescribed dose and duration (n = 2). Examples included prescribing opioids during pregnancy, concurrently with benzodiazepines, long-term without a laxative prescription and prescribing > 120-mg morphine milligram equivalent per day or long-term duration over 3 months after surgery.
The high agreement on opioid prescribing indicators indicates that these potentially hazardous consequences are relevant and concerning to healthcare practitioners. Future research is needed to evaluate the feasibility and implementation of these indicators within primary care settings. This research will provide valuable insights and evidence to support opioid prescribing and deprescribing strategies. Moreover, the findings will be crucial in informing primary care practitioners and shaping quality outcome frameworks and other initiatives to enhance the safety and quality of care in primary care settings.
长期使用阿片类药物会导致依赖、成瘾和严重的不良事件。尽管已经存在一个减少不合理阿片类药物处方的框架,但在英国的初级保健中,对于慢性疼痛患者可预防的阿片类药物相关问题的处方指标,尚未达成共识。本研究旨在确定阿片类药物处方指标的处方场景,以制定用于慢性疼痛患者阿片类药物处方的指标。
从文献综述、指南和政府报告中确定了阿片类药物处方指标的场景。确定了 21 个指标,并在涉及阿片类药物相关危害和不良反应、药物相互作用以及特定疾病条件下的药物-疾病相互作用的各种阿片类药物场景中呈现。在获得伦理批准后,于 2020 年 8 月至 2021 年 2 月,使用来自英国的 24 名专家(临床医生、药剂师和独立处方者)进行了两轮电子德尔菲小组技术调查。每个指标的评分范围为 1-9,从不合适到合适。计算了中位数、第 30 百分位和第 70 百分位以及分歧指数。
小组一致认为 21 个阿片类药物处方场景中的 15 个场景是不合适的,主要是因为它们可能对患者造成伤害。这一共识反映在低适宜性评分(中位数范围为 1-3)中。没有一个场景被认为是高度一致的,即处方是合适的。这些指标被认为不合适,原因是药物-疾病相互作用(n=8)、药物-药物相互作用(n=2)、不良反应(n=3)和规定的剂量和持续时间(n=2)。例如,在怀孕期间、同时开苯二氮䓬类药物、长期不开用泻药、每天处方超过 120 毫克吗啡毫克当量或手术后长期持续 3 个月以上。
在阿片类药物处方指标上的高度一致表明,这些潜在的危险后果与医疗保健从业者有关且值得关注。需要进一步研究来评估这些指标在初级保健环境中的可行性和实施情况。这项研究将提供有价值的见解和证据,以支持阿片类药物的处方和停药策略。此外,研究结果对于指导初级保健医生以及制定质量结果框架和其他举措,以提高初级保健环境中的安全性和护理质量至关重要。