Department of Cardiology and Pneumology, University Medical Center Göttingen, Georg-August-University Göttingen, Robert-Koch-Str. 40, 37099, Göttingen, Germany.
German Center for Cardiovascular Research (DZHK), Partner Site Göttingen, Göttingen, Germany.
Clin Res Cardiol. 2024 Mar;113(3):496-508. doi: 10.1007/s00392-023-02363-5. Epub 2024 Jan 3.
The diagnosis of heart failure with preserved ejection fraction (HFpEF) remains challenging. Recently, the HFpEF Stress Trial demonstrated feasibility and accuracy of non-invasive cardiovascular magnetic resonance (CMR) real-time (RT) exercise-stress atrial function imaging for early identification of HFpEF. However, no outcome data have yet been presented.
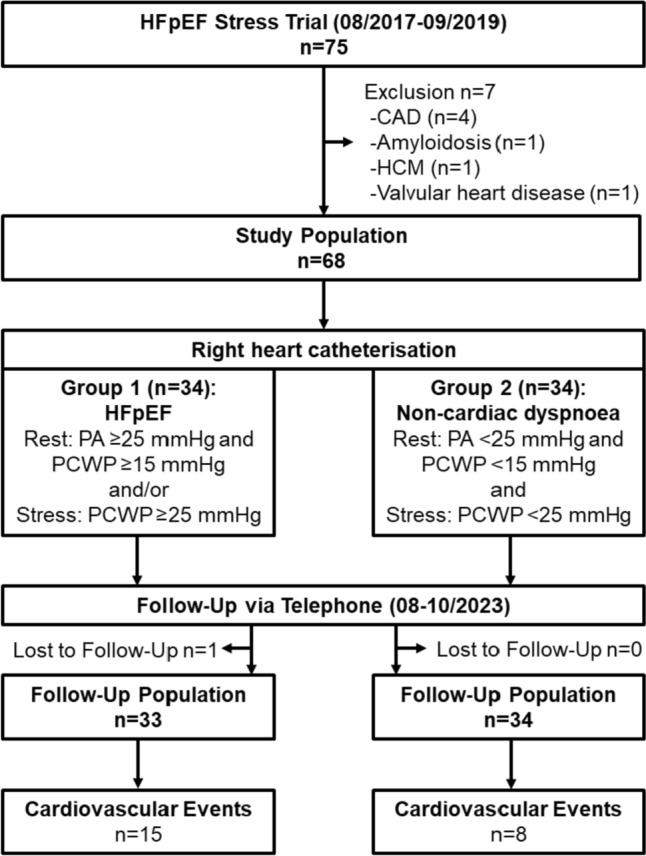
The HFpEF Stress Trial (DZHK-17) prospectively recruited 75 patients with dyspnea on exertion and echocardiographic preserved EF and signs of diastolic dysfunction (E/e' > 8). 68 patients entered the final study cohort and were characterized as HFpEF (n = 34) or non-cardiac dyspnea (n = 34) according to pulmonary capillary wedge pressure (HFpEF: PCWP rest: ≥ 15 mmHg stress: ≥ 25 mmHg). These patients were contacted by telephone and hospital charts were reviewed. The clinical endpoint was cardiovascular events (CVE).
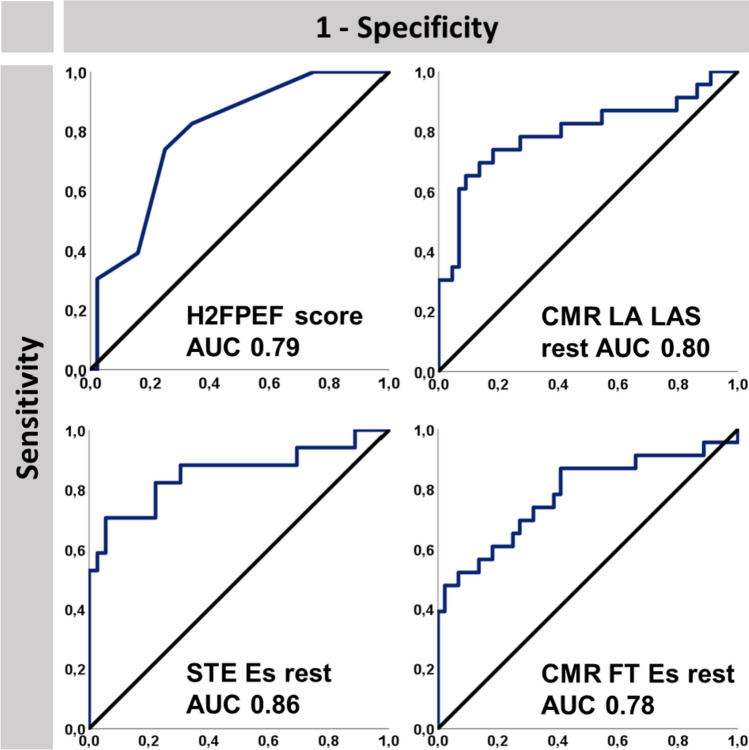
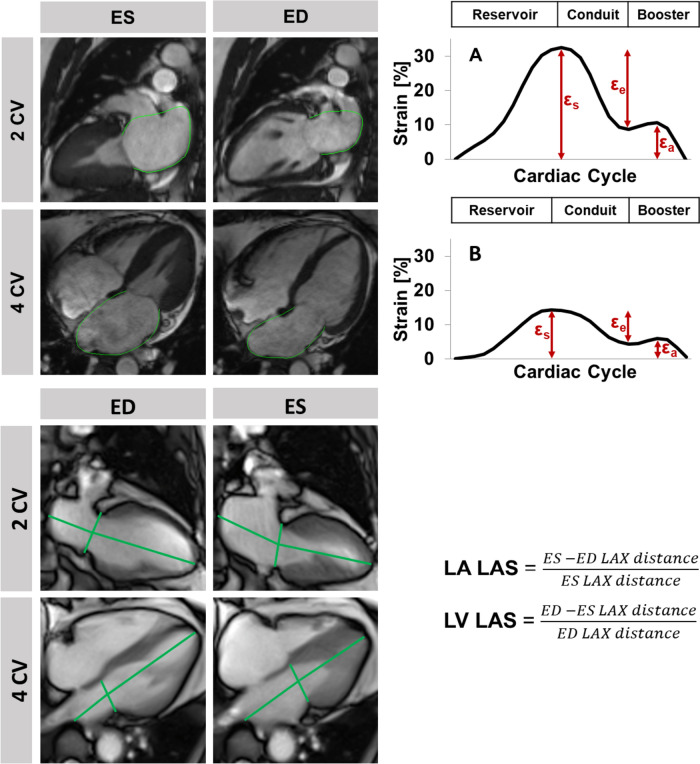
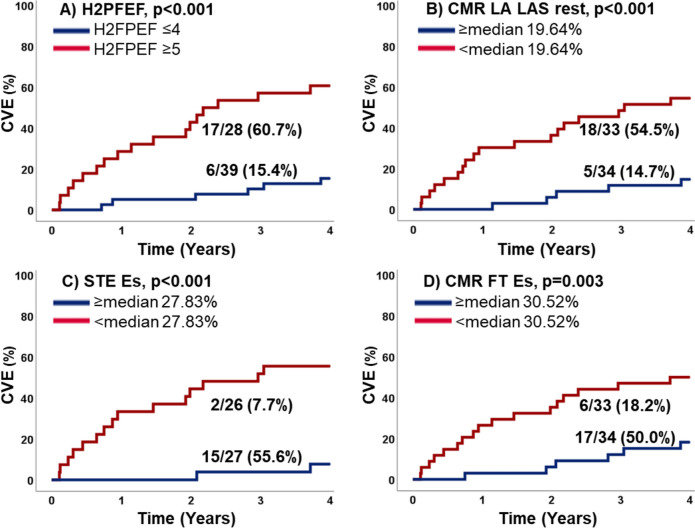
Follow-up was performed after 48 months; 1 patient was lost to follow-up. HFpEF patients were more frequently compared to non-cardiac dyspnea (15 vs. 8, p = 0.059). Hospitalised patients during follow-up had higher H2FPEF scores (5 vs. 3, p < 0.001), and impaired left atrial (LA) function at rest (p ≤ 0.002) and stress (p ≤ 0.006). Impairment of CMR-derived atrial function parameters at rest and during exercise-stress (p ≤ 0.003) was associated with increased likelihood for CVE. CMR-Feature Tracking LA Es/Ee (p = 0.016/0.017) and RT-CMR derived LA long axis strain (p = 0.003) were predictors of CVE independent of the presence of atrial fibrillation.
Left atrial function emerged as the strongest predictor for 4-year outcome in the HFpEF Stress Trial. A combination of rest and exercise-stress LA function quantification allows accurate diagnostic and prognostic stratification in HFpEF.
gov: NCT03260621.
射血分数保留的心力衰竭(HFpEF)的诊断仍然具有挑战性。最近,HFpEF 应激试验证明了非侵入性心血管磁共振(CMR)实时(RT)运动应激心房功能成像在早期识别 HFpEF 方面的可行性和准确性。然而,目前还没有相关的预后数据。
HFpEF 应激试验(DZHK-17)前瞻性招募了 75 例劳力性呼吸困难且超声心动图显示射血分数保留和舒张功能障碍迹象(E/e' > 8)的患者。68 例患者进入最终的研究队列,并根据肺毛细血管楔压(HFpEF:PCWP 静息时:≥ 15mmHg,应激时:≥ 25mmHg)将其特征为 HFpEF(n = 34)或非心源性呼吸困难(n = 34)。通过电话联系这些患者,并回顾医院病历。临床终点是心血管事件(CVE)。
随访 48 个月后,有 1 例患者失访。与非心源性呼吸困难患者相比,HFpEF 患者更常见(15 例 vs. 8 例,p = 0.059)。随访期间住院的患者 H2FPEF 评分更高(5 分 vs. 3 分,p < 0.001),静息和应激时左心房(LA)功能受损(p ≤ 0.002)。静息和运动应激时 CMR 衍生的心房功能参数受损(p ≤ 0.003)与 CVE 的发生几率增加相关。CMR-Feature Tracking LA Es/Ee(p = 0.016/0.017)和 RT-CMR 衍生的 LA 长轴应变(p = 0.003)是独立于心房颤动存在的 CVE 的预测因素。
左心房功能是 HFpEF 应激试验 4 年预后的最强预测因素。静息和运动应激时 LA 功能定量相结合可准确诊断和分层 HFpEF 患者的预后。
gov:NCT03260621。