Nassal Michelle M J, Wang Henry E, Benoit Justin L, Kuhn Alexander, Powell Jonathan R, Keseg David, Sauto James, Panchal Ashish R
Department of Emergency Medicine, The Ohio State University, Columbus, OH, United States.
Department of Emergency Medicine, University of Cincinnati, Cincinnati, OH, United States.
Resusc Plus. 2023 Dec 16;17:100528. doi: 10.1016/j.resplu.2023.100528. eCollection 2024 Mar.
Public health surveillance is essential for improving community health. The Cardiac Arrest Registry to Enhance Survival (CARES) is a surveillance system for out-of-hospital cardiac arrest (OHCA). We describe results of the organized statewide implementation of Ohio CARES.
We performed a retrospective analysis of CARES enactment in Ohio. Key elements included: establishment of statewide leadership, appointment of a dedicated coordinator, conversion to a statewide subscription, statewide dissemination of information, fundraising from internal and external stakeholders, and conduct of resuscitation academies. We identified all adult (≥18 years) OHCA reported in the registry during 2013-2020. We evaluated OHCA characteristics before (2013-2015) and after (2016-2019) statewide implementation using chi-square test. We evaluated trends in OHCA outcomes using the Cochran-Armitage test of trend.
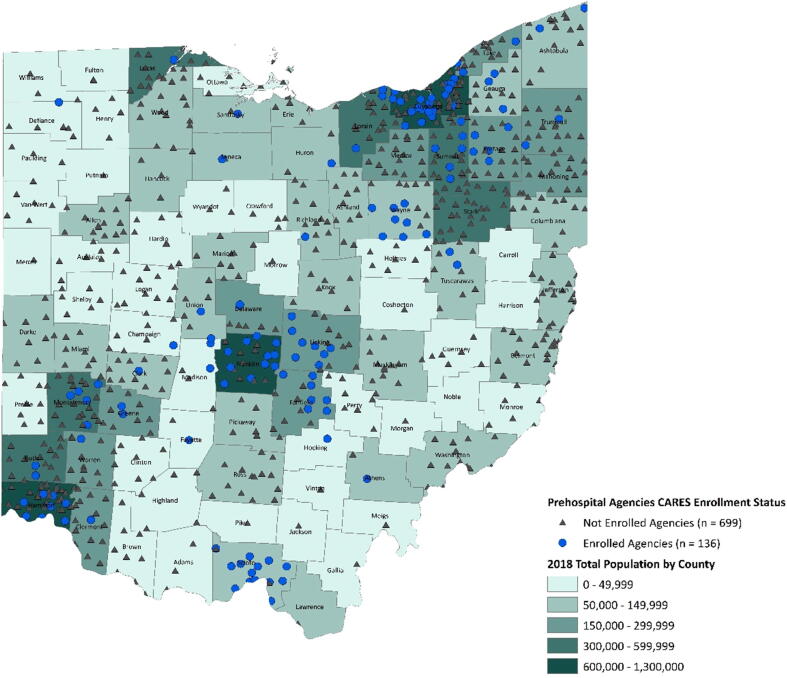
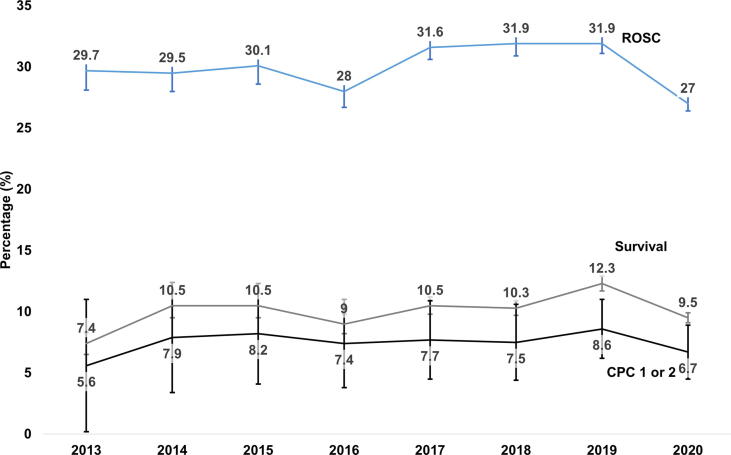
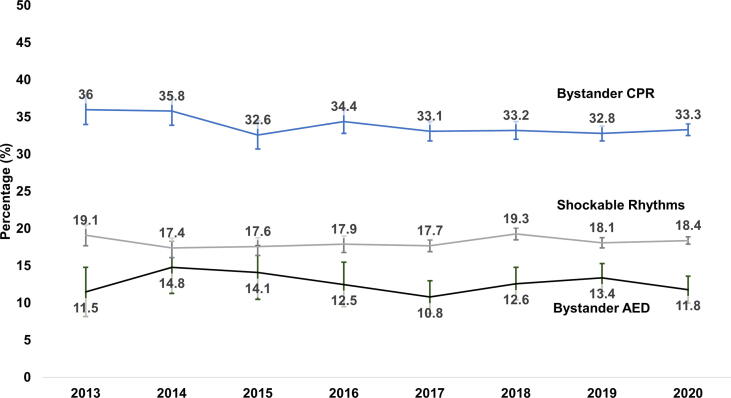
Statewide CARES promotion increased participation from 2 (urban) to 136 (129 urban, 7 rural) EMS agencies. Covered population increased from 1.2 M (10% of state) to 4.8 M (41% of state). After statewide implementation, OHCA populations increased male (58.1% vs 60.8%, p < 0.01), white (50.1% vs 63.7%, p < 0.01), bystander witnessed (26.9% vs 32.9%, p < 0.01) OHCAs. Bystander CPR (34.7% vs 33.2%, p = 0.22), bystander AED (13.5% vs 12.3%, p = 0.55) and initial rhythm (shockable 18.0% vs 18.3%, p = 0.32) did not change. From 2013 to 2019 there were temporal increases in ROSC (29.7% to 31.9%, p-trend = 0.028), survival (7.4% to 12.3%, p-trend < 0.001) and survival with good neurologic outcome (5.6% to 8.6%, p-trend = 0.047).
The organized statewide implementation of CARES in Ohio was associated with marked increases in community uptake and concurrent observed improvements in patient outcomes. These results highlight key lessons for community-wide fostering of OHCA surveillance.
公共卫生监测对于改善社区健康至关重要。心脏骤停增强生存登记系统(CARES)是一个院外心脏骤停(OHCA)监测系统。我们描述了俄亥俄州CARES在全州范围内有组织实施的结果。
我们对俄亥俄州CARES的实施情况进行了回顾性分析。关键要素包括:建立全州范围内的领导机构、任命一名专职协调员、转变为全州范围内的订阅模式、在全州范围内传播信息、从内部和外部利益相关者那里筹集资金以及举办复苏学院。我们确定了2013 - 2020年登记册中报告的所有成年(≥18岁)OHCA病例。我们使用卡方检验评估了全州实施之前(2013 - 2015年)和之后(2016 - 2019年)OHCA的特征。我们使用 Cochr an - Armitage趋势检验评估了OHCA结局的趋势。
全州范围内对CARES的推广使参与的急救医疗服务(EMS)机构从2个(城市)增加到136个(129个城市,7个农村)。覆盖人口从120万(占该州的10%)增加到480万(占该州的41%)。在全州实施之后,OHCA人群中男性(58.1%对60.8%,p < 0.01)、白人(50.1%对63.7%,p < 0.01)、有旁观者目睹的OHCA(26.9%对32.9%,p < 0.01)的比例有所增加。旁观者进行心肺复苏(CPR)(34.7%对33.2%,p = 0.22)、旁观者使用自动体外除颤器(AED)(13.5%对12.3%,p = 0.55)以及初始心律(可电击心律18.0%对18.3%,p = 0.32)没有变化。从2013年到2019年,自主循环恢复(ROSC)(29.7%至31.9%,p趋势 = 0.028)、生存(7.4%至12.3%,p趋势 < 0.001)以及有良好神经学结局的生存(5.6%至8.6%,p趋势 = 0.047)在时间上有所增加。
俄亥俄州对CARES进行全州范围内的有组织实施与社区参与的显著增加以及同时观察到的患者结局改善相关。这些结果突出了在社区范围内促进OHCA监测方面的关键经验教训。