From the Division of Neurology (H.S.N., F.Z., Y.Z., H.T.), Department of Medicine and the Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver, Canada; Flinders Health and Medical Research Institute (H.S.N.), College of Medicine and Public Health, Flinders University, Adelaide, Australia; SA Pharmacy (H.S.N.), Northern and Southern Adelaide Local Health Networks, Australia; College of Pharmacy and Nutrition (S.Y., C.E.), University of Saskatchewan; Saskatchewan Health Quality Council (S.Y., X.L.), Saskatoon; Department of Community Health Sciences (O.E.), Rady Faculty of Health Sciences, University of Manitoba, Winnipeg; Nova Scotia Health and the Departments of Psychiatry, Psychology and Neuroscience, and Medicine (J.D.F.), Dalhousie University, Halifax; and Departments of Internal Medicine and Community Health Sciences (R.A.M.), Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, Canada.
Neurology. 2024 Feb 13;102(3):e208006. doi: 10.1212/WNL.0000000000208006. Epub 2024 Jan 5.
It is not possible to fully establish the safety of a disease-modifying drug (DMD) for multiple sclerosis (MS) from randomized controlled trials as only very common adverse events occurring over the short-term can be captured, and the quality of reporting has been variable. We examined the relationship between the DMDs for MS and potential adverse events in a multiregion population-based study.
We identified people with MS using linked administrative health data from 4 Canadian provinces. MS cases were followed from the most recent of first MS or related demyelinating disease event on January 1, 1996, until the earliest of emigration, death, or December 31, 2017. DMD exposure primarily comprised β-interferon, glatiramer acetate, natalizumab, fingolimod, dimethyl fumarate, teriflunomide, and alemtuzumab. We examined associations between DMD exposure and infection-related hospitalizations and physician visits using recurrent events proportional means models and between DMD exposure and 15 broad categories of incident adverse events using stratified multivariate Cox proportional hazard models.
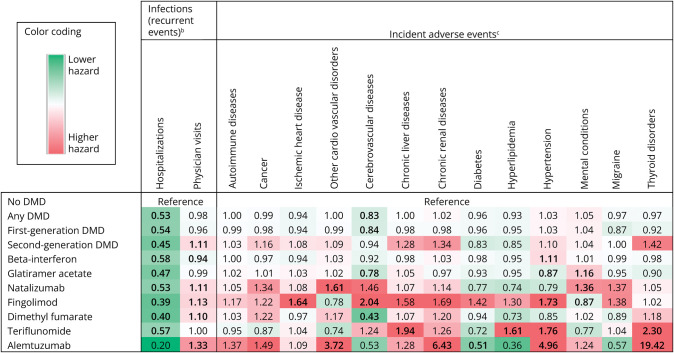
We identified 35,894 people with MS. While virtually all DMDs were associated with a 42%-61% lower risk of infection-related hospitalizations, there was a modest increase in infection-related physician visits by 10%-33% for select DMDs. For incident adverse events, most elevated risks involved a second-generation DMD, with alemtuzumab's hazard of thyroid disorders being 19.42 (95% CI 9.29-36.51), hypertension 4.96 (95% CI 1.78-13.84), and cardiovascular disease 3.72 (95% CI 2.12-6.53). Natalizumab's highest risk was for cardiovascular disease (adjusted hazard ratio [aHR] 1.61; 95% CI 1.24-2.10). For the oral DMDs, fingolimod was associated with higher hazards of cerebrovascular (aHR 2.04; 95% CI 1.27-3.30) and ischemic heart diseases (aHR 1.64; 95% CI 1.10-2.44) and hypertension (aHR 1.73; 95% CI 1.30-2.31); teriflunomide with higher hazards of thyroid disorders (aHR 2.30; 95% CI 1.11-4.74), chronic liver disease (aHR 1.94; 95% CI 1.19-3.18), hypertension (aHR 1.76; 95% CI 1.32-2.37), and hyperlipidemia (aHR 1.61; 95% CI 1.07-2.44); and from complementary analyses (in 1 province), dimethyl fumarate with acute liver injury (aHR 6.55; 95% CI 1.96-21.87).
Our study provides an extensive safety profile of several different DMDs used to treat MS in the real-world setting. Our findings not only complement those observed in short-term clinical trials but also provide new insights that help inform the risk-benefit profile of the DMDs used to treat MS in clinical practice. The results of this study highlight the continued need for long-term, independent safety studies of the DMDs used to treat MS.
This study provides Class III evidence that for patients with MS, while DMD exposure reduces the risk of infection-related hospitalizations, there are increased risks of infection-related physician visits and incident adverse events for select DMDs.
由于只能捕获短期发生的常见不良事件,因此从随机对照试验中不可能完全确定多发性硬化症(MS)的疾病修饰药物(DMD)的安全性,并且报告的质量也存在差异。我们在一项多区域基于人群的研究中检查了 MS 的 DMD 与潜在不良事件之间的关系。
我们使用来自加拿大 4 个省的链接行政健康数据来识别 MS 患者。从 1996 年 1 月 1 日最近的首次 MS 或相关脱髓鞘疾病事件开始,对 MS 病例进行随访,直到最早的移民、死亡或 2017 年 12 月 31 日。DMD 暴露主要包括β干扰素、聚乙二醇干扰素、那他珠单抗、芬戈莫德、二甲基富马酸、特立氟胺和阿仑单抗。我们使用复发事件比例均值模型检查 DMD 暴露与感染相关住院和医生就诊之间的关联,使用分层多变量 Cox 比例风险模型检查 DMD 暴露与 15 个广泛类别的新发不良事件之间的关联。
我们确定了 35894 名 MS 患者。虽然几乎所有的 DMD 都与 42%-61%的较低感染相关住院风险相关,但对于某些 DMD,感染相关医生就诊的风险略有增加,增加了 10%-33%。对于新发不良事件,大多数风险较高的事件涉及第二代 DMD,其中阿仑单抗的甲状腺疾病风险为 19.42(95%CI 9.29-36.51),高血压为 4.96(95%CI 1.78-13.84),心血管疾病为 3.72(95%CI 2.12-6.53)。那他珠单抗的最高风险是心血管疾病(调整后的危险比[aHR]1.61;95%CI 1.24-2.10)。对于口服 DMD,芬戈莫德与更高的脑血管病(aHR 2.04;95%CI 1.27-3.30)和缺血性心脏病(aHR 1.64;95%CI 1.10-2.44)和高血压(aHR 1.73;95%CI 1.30-2.31)的风险相关;特立氟胺与更高的甲状腺疾病(aHR 2.30;95%CI 1.11-4.74)、慢性肝病(aHR 1.94;95%CI 1.19-3.18)、高血压(aHR 1.76;95%CI 1.32-2.37)和高血脂(aHR 1.61;95%CI 1.07-2.44)的风险相关;从补充分析(在一个省),二甲基富马酸与急性肝损伤(aHR 6.55;95%CI 1.96-21.87)的风险相关。
我们的研究提供了几种不同的 DMD 用于治疗 MS 的广泛安全性概况。我们的研究结果不仅补充了短期临床试验中的观察结果,而且还提供了新的见解,有助于为治疗 MS 的 DMD 在临床实践中的风险效益概况提供信息。这项研究的结果强调了继续进行长期、独立的 DMD 安全性研究的必要性。
这项研究提供了 III 级证据,对于患有 MS 的患者,虽然 DMD 暴露降低了感染相关住院的风险,但对于某些 DMD,感染相关医生就诊和新发不良事件的风险增加。