Department of Hematology, CHU de Rennes, Rennes, France.
Etablissement français du sang Bretagne, Rennes, France.
Blood Adv. 2024 Mar 26;8(6):1573-1585. doi: 10.1182/bloodadvances.2023011727.
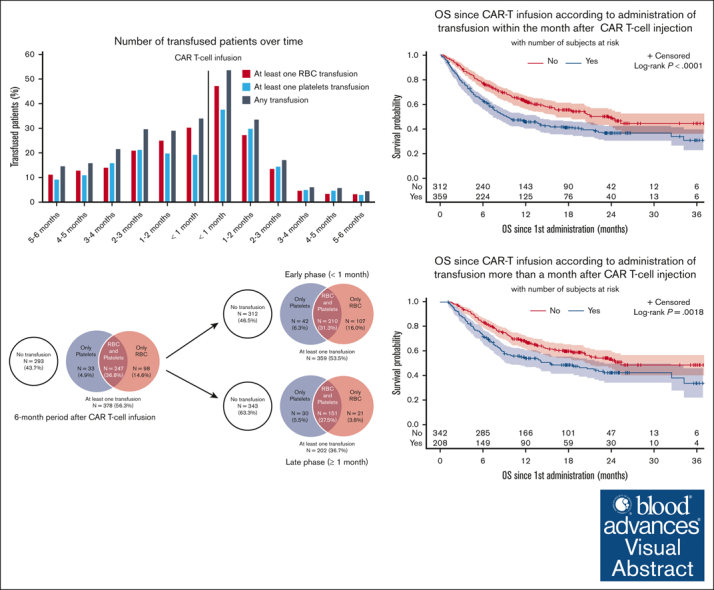
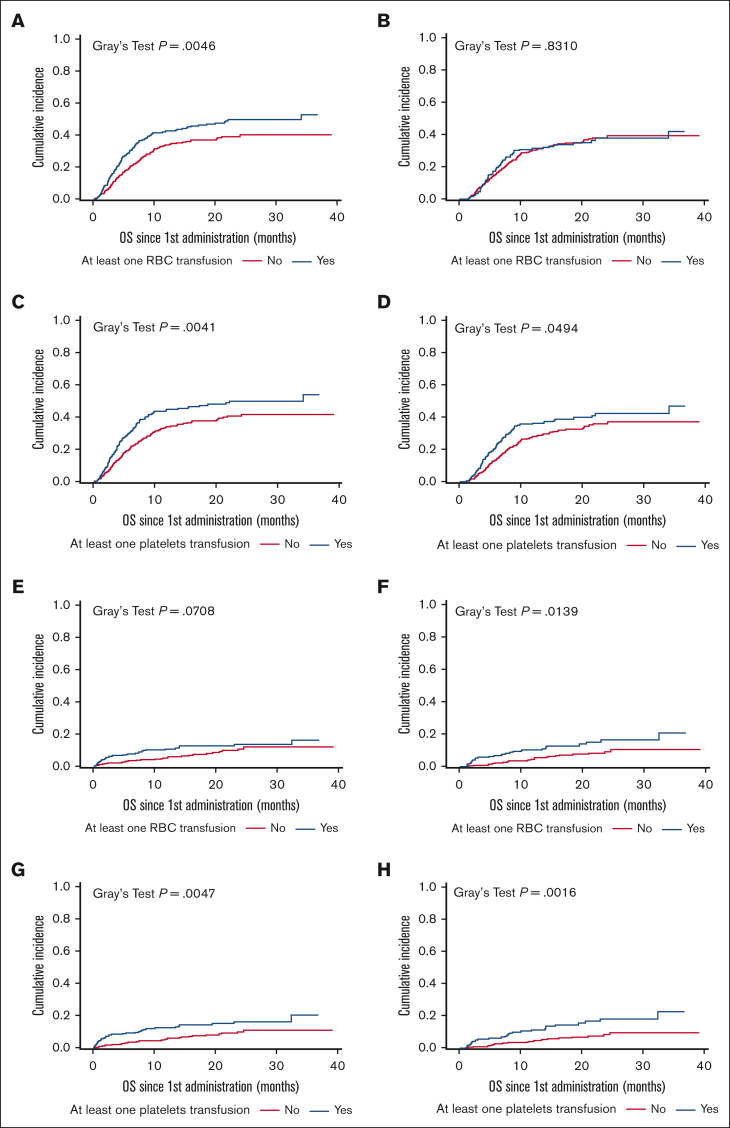
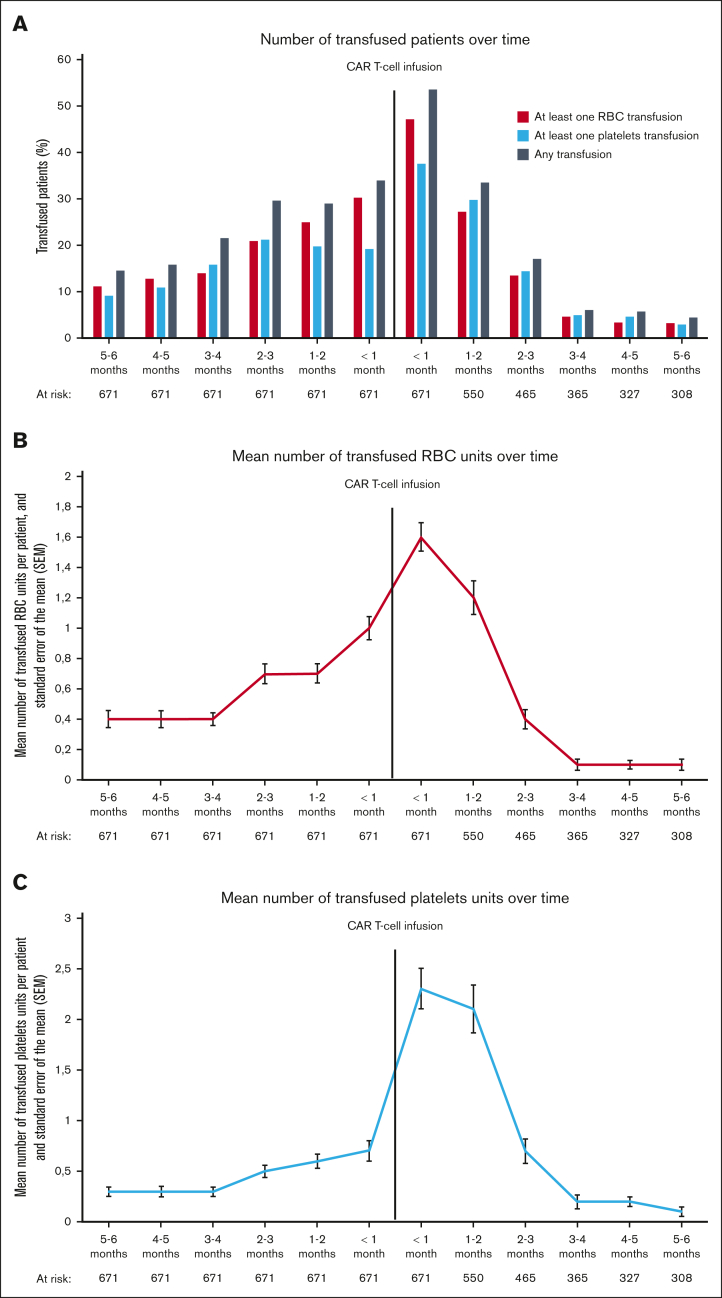
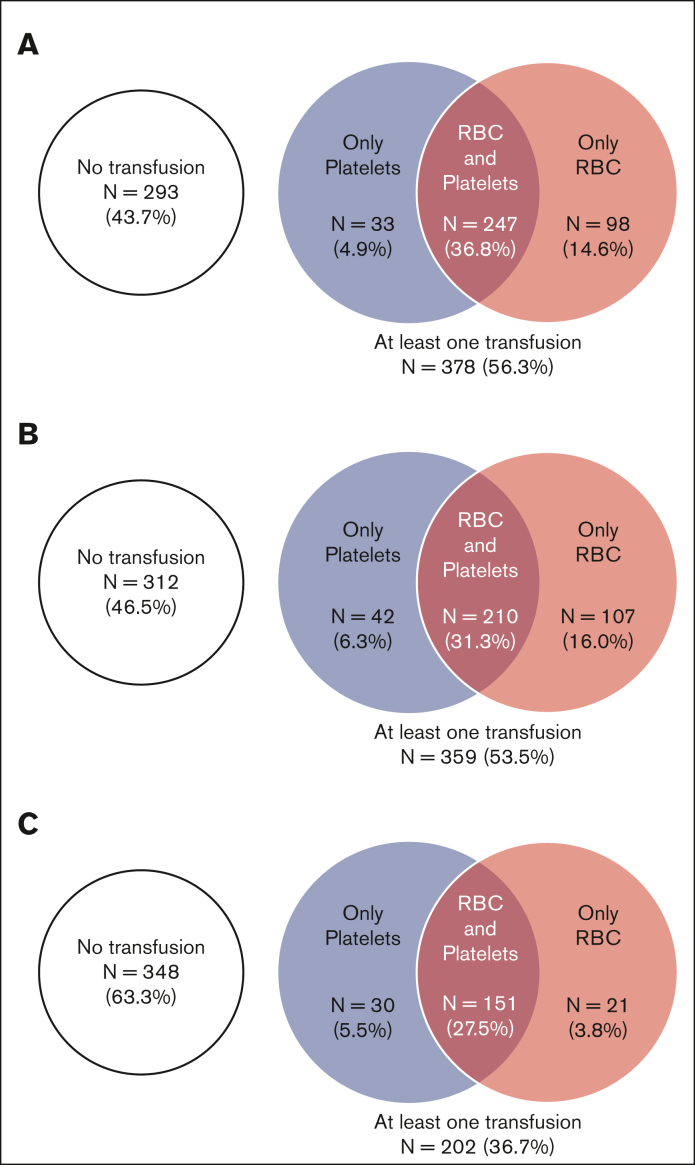
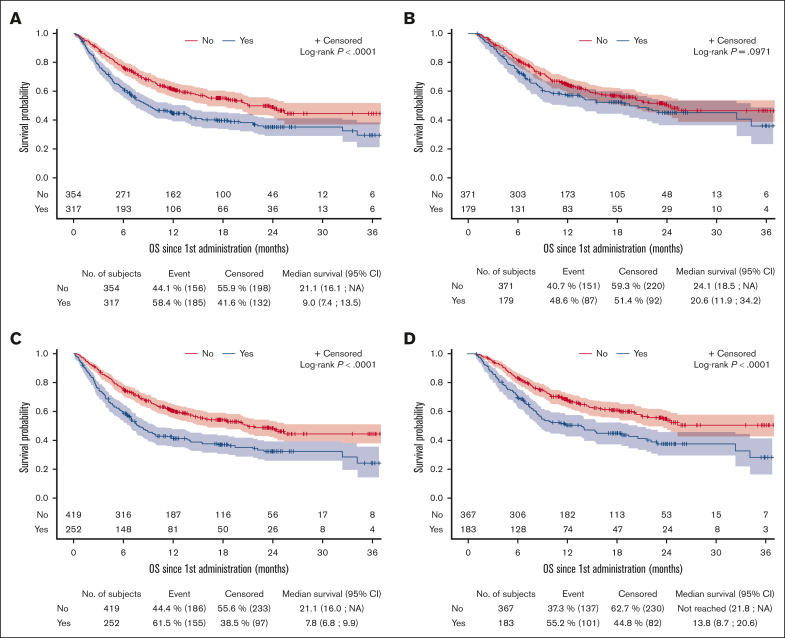
Chimeric antigen receptor (CAR) T-cells targeting CD19 have been approved for the treatment of relapse/refractory large B-cell lymphoma. Hematotoxicity is the most frequent CAR T-cell-related adverse event. Transfusion support is a surrogate marker of severe cytopenias. Transfusion affects patients' quality of life, presents specific toxicities, and is known to affect immunity through the so-called transfusion-related immunomodulation that may affect CAR T-cell efficacy. We analyzed data from 671 patients from the French DESCAR-T registry for whom exhaustive transfusion data were available. Overall, 401 (59.8%) and 378 (56.3%) patients received transfusion in the 6-month period before and after CAR T-cell infusion, respectively. The number of patients receiving transfusion and the mean number of transfused products increased during the 6-month period before CAR T-cell infusion, peaked during the first month after infusion (early phase), and decreased over time. Predictive factors for transfusion at the early phase were age >60 years, ECOG PS ≥2, treatment with axicabtagene ciloleucel, pre-CAR T-cell transfusions, and CAR-HEMATOTOX score ≥2. Predictive factors for late transfusion (between 1 and 6 months after infusion) were pre-CAR T-cell transfusions, CAR-HEMATOTOX score ≥2, ICANS ≥3 (for red blood cells [RBC] transfusion), and tocilizumab use (for platelets transfusion). Early transfusions and late platelets (but not RBC) transfusions were associated with a shorter progression-free survival and overall survival. Lymphoma-related mortality and nonrelapse mortality were both increased in the transfused population. Our data shed light on the mechanisms of early and late cytopenia and on the potential impact of transfusions on CAR T-cell efficacy and toxicity.
嵌合抗原受体(CAR)T 细胞靶向 CD19 已被批准用于治疗复发/难治性大 B 细胞淋巴瘤。血液毒性是最常见的 CAR T 细胞相关不良事件。输血支持是严重细胞减少症的替代标志物。输血会影响患者的生活质量,带来特定的毒性,并且已知通过所谓的输血相关免疫调节来影响免疫,这可能会影响 CAR T 细胞的疗效。我们分析了法国 DESCAR-T 注册中心 671 名患者的数据,这些患者有详尽的输血数据。总体而言,分别有 401(59.8%)和 378(56.3%)名患者在 CAR T 细胞输注前 6 个月和输注后 6 个月接受了输血。在 CAR T 细胞输注前的 6 个月内,接受输血的患者数量和输注的产品数量均增加,在输注后第一个月(早期)达到峰值,随后逐渐减少。早期输血的预测因素为年龄>60 岁、ECOG PS≥2、接受 axicabtagene ciloleucel 治疗、输注前输血和 CAR-HEMATOTOX 评分≥2。晚期输血(输注后 1 至 6 个月)的预测因素为输注前输血、CAR-HEMATOTOX 评分≥2、ICANS≥3(红细胞 [RBC] 输血)和使用托珠单抗(血小板输血)。早期输血和晚期血小板(而非 RBC)输血与较短的无进展生存期和总生存期相关。输血患者的淋巴瘤相关死亡率和非复发死亡率均升高。我们的数据阐明了早期和晚期细胞减少症的机制,以及输血对 CAR T 细胞疗效和毒性的潜在影响。