Valls-Esteve Arnau, Tejo-Otero Aitor, Adell-Gómez Núria, Lustig-Gainza Pamela, Fenollosa-Artés Felip, Buj-Corral Irene, Rubio-Palau Josep, Munuera Josep, Krauel Lucas
Innovation Department, SJD Barcelona Children's Hospital, Santa Rosa 39-57, 08950 Esplugues de Llobregat, Spain.
Medicina i Recerca Translacional, Facultat de Medicina i Ciències de la Salut, Universitat de Barcelona, 08007 Barcelona, Spain.
Bioengineering (Basel). 2023 Dec 27;11(1):31. doi: 10.3390/bioengineering11010031.
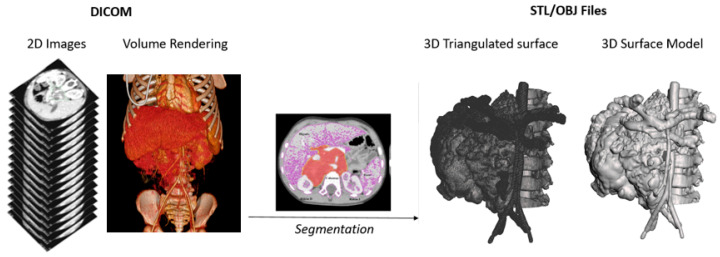
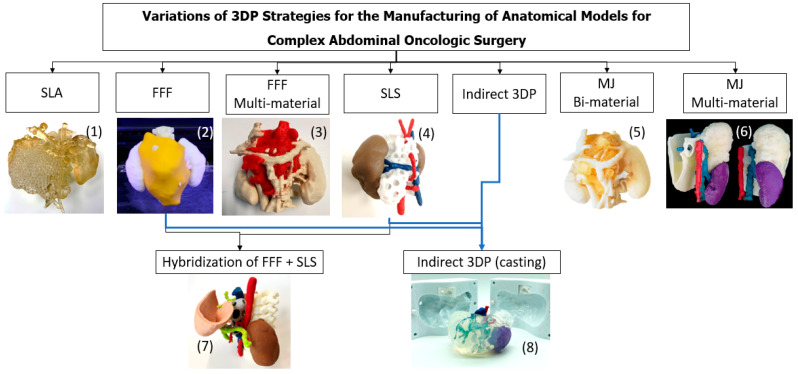
The printing and manufacturing of anatomical 3D models has gained popularity in complex surgical cases for surgical planning, simulation and training, the evaluation of anatomical relations, medical device testing and patient-professional communication. 3D models provide the haptic feedback that Virtual or Augmented Reality (VR/AR) cannot provide. However, there are many technologies and strategies for the production of 3D models. Therefore, the aim of the present study is to show and compare eight different strategies for the manufacture of surgical planning and training prototypes. The eight strategies for creating complex abdominal oncological anatomical models, based on eight common pediatric oncological cases, were developed using four common technologies (stereolithography (SLA), selectie laser sinterning (SLS), fused filament fabrication (FFF) and material jetting (MJ)) along with indirect and hybrid 3D printing methods. Nine materials were selected for their properties, with the final models assessed for application suitability, production time, viscoelastic mechanical properties (shore hardness and elastic modulus) and cost. The manufacturing and post-processing of each strategy is assessed, with times ranging from 12 h (FFF) to 61 h (hybridization of FFF and SLS), as labor times differ significantly. Cost per model variation is also significant, ranging from EUR 80 (FFF) to EUR 600 (MJ). The main limitation is the mimicry of physiological properties. Viscoelastic properties and the combination of materials, colors and textures are also substantially different according to the strategy and the intended use. It was concluded that MJ is the best overall option, although its use in hospitals is limited due to its cost. Consequently, indirect 3D printing could be a solid and cheaper alternative.
解剖3D模型的打印和制造在复杂手术病例的手术规划、模拟和训练、解剖关系评估、医疗设备测试以及医患沟通方面越来越受欢迎。3D模型提供了虚拟现实或增强现实(VR/AR)无法提供的触觉反馈。然而,3D模型制作有许多技术和策略。因此,本研究的目的是展示和比较八种不同的手术规划和训练原型制造策略。基于八个常见的儿科肿瘤病例,使用四种常见技术(立体光刻(SLA)、选择性激光烧结(SLS)、熔融沉积成型(FFF)和材料喷射(MJ))以及间接和混合3D打印方法,开发了创建复杂腹部肿瘤解剖模型的八种策略。根据材料特性选择了九种材料,对最终模型的应用适用性、制作时间、粘弹性力学性能(邵氏硬度和弹性模量)和成本进行了评估。评估了每种策略的制造和后处理过程,时间从12小时(FFF)到61小时(FFF和SLS混合)不等,因为人工时间差异很大。每个模型的成本差异也很大,从80欧元(FFF)到600欧元(MJ)不等。主要限制在于生理特性的模拟。根据策略和预期用途,粘弹性性能以及材料、颜色和纹理的组合也有很大差异。得出的结论是,MJ总体上是最佳选择,尽管由于成本原因其在医院的使用受到限制。因此,间接3D打印可能是一种可靠且成本较低的替代方案。