Rufa Magdalena, Nagib Ragi, Aktuerk Dincer, Ahad Samir, Ghinescu Mihnea, Franke Ulrich
Department of Cardiovascular Surgery, Robert Bosch Hospital, Stuttgart, Germany.
Barts Heart Centre, Barts Health NHS, London, UK.
J Thorac Dis. 2023 Dec 30;15(12):6459-6474. doi: 10.21037/jtd-23-1306. Epub 2023 Dec 5.
Atrial fibrillation (AF) occurs frequently in patients with mitral valve disease. Results of cryoablation concomitant with either minimally invasive video-assisted [minimally invasive mitral valve surgery (MIMVS)] or with robotic-assisted (RMV) mitral valve surgery have previously been separately reported. However, there are up-to-date no studies comparing the two procedures in terms of safety, efficacy, and mid-term follow-up.
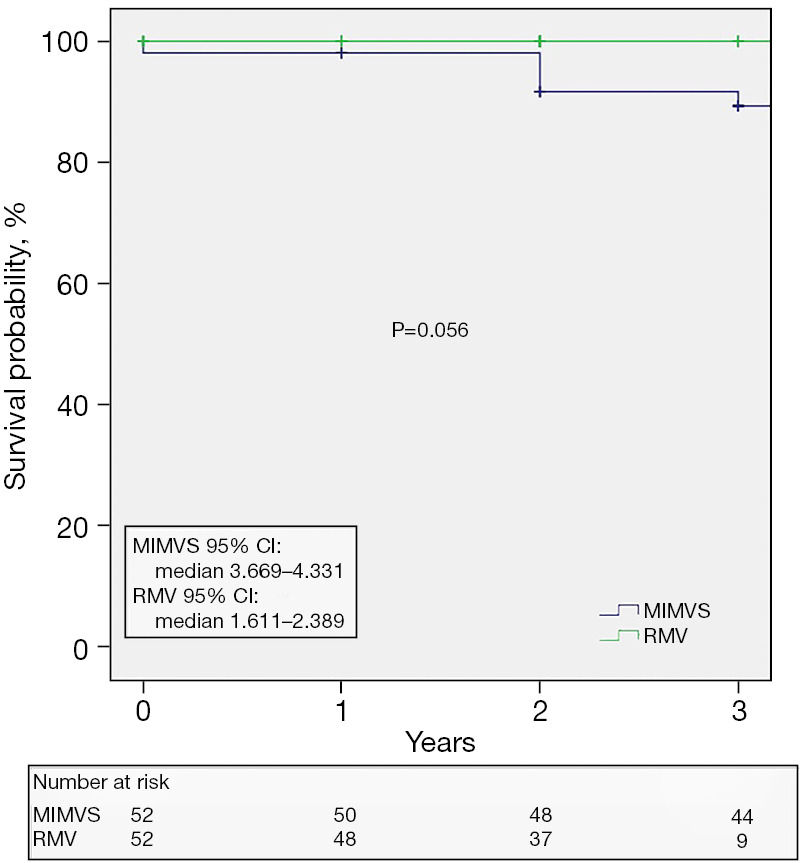
Between January 2017 and March 2022, 294 patients underwent MIMVS, and 187 patients underwent RMV at our institution. After 1:1 propensity score matching using 22 preoperative variables, the study included 104 patients. Group 1 (MIMVS) included 52 patients operated on between 2017-2022 using a minimally invasive video-assisted right-sided mini-thoracotomy. Group 2 (RMV) included 52 patients operated on between 2019-2021 using a robotic-assisted approach. Early and mid-term outcomes were assessed, including maintenance of sinus rhythm. Follow-up was 100% complete at a median follow-up of 2 years.
For the entire propensity matched cohort, the median EuroSCORE II was 3.14 [interquartile range (IQR), 1.93-4.99], the median age was 68 (IQR, 61-74) years, and two thirds of the patients were male. Most (72.1%) underwent mitral valve surgery, and 26.9% had an additional tricuspid procedure. Only four patients underwent mitral valve replacement (3.8%). The majority (87.5%) received a left-sided atrial Maze and 12.5% a bi-atrial Maze. The left atrial appendage was occluded in 72.1% cases. Overall, there were no significant differences between the two propensity matched groups in baseline demographics or intra-operative characteristics. Similarly, there were no significant differences in the post-operative short and mid-term outcomes between the two groups. There were no in-hospital or 30-day deaths. At the mid-term survival was similar between groups, log-rank test P=0.056. Maintenance of sinus rhythm at follow-up was 76%.
Mitral or double valve repair with concomitant cryoablation can be safely performed with either a MIMVS or RMV approach. Both methods demonstrated outstanding early and mid-term outcomes.
心房颤动(AF)在二尖瓣疾病患者中频繁发生。此前已分别报道了与微创电视辅助(微创二尖瓣手术(MIMVS))或机器人辅助(RMV)二尖瓣手术同时进行的冷冻消融结果。然而,目前尚无关于这两种手术在安全性、有效性和中期随访方面进行比较的研究。
2017年1月至2022年3月期间,294例患者在我院接受了MIMVS,187例患者接受了RMV。在使用22个术前变量进行1:1倾向评分匹配后,该研究纳入了104例患者。第1组(MIMVS)包括52例在2017 - 2022年期间采用微创电视辅助右侧小切口开胸手术的患者。第2组(RMV)包括52例在2019 - 2021年期间采用机器人辅助方法手术的患者。评估了早期和中期结果,包括窦性心律的维持情况。随访在中位随访2年时100%完成。
对于整个倾向匹配队列,欧洲心脏手术风险评估系统(EuroSCORE)II中位数为3.14[四分位间距(IQR),1.93 - 4.99],中位年龄为68岁(IQR,61 - 74岁),三分之二的患者为男性。大多数(72.1%)接受了二尖瓣手术,26.9%进行了额外的三尖瓣手术。仅4例患者接受了二尖瓣置换术(3.8%)。大多数(87.5%)接受了左侧心房迷宫手术,12.5%接受了双心房迷宫手术。72.1%的病例闭塞了左心耳。总体而言,两个倾向匹配组在基线人口统计学或术中特征方面无显著差异。同样,两组术后短期和中期结果也无显著差异。无院内死亡或30天死亡。中期两组生存率相似,对数秩检验P = 0.056。随访时窦性心律维持率为76%。
二尖瓣或双瓣膜修复同时进行冷冻消融,采用MIMVS或RMV方法均可安全实施。两种方法均显示出出色的早期和中期结果。