Zhang Qihao, Xu Erhe, Li Hai-Feng, Chan Piu, Zhao Zhenzhen, Ma Jinghong
Department of Neurology, Xuanwu Hospital, Capital Medical University, Beijing, China.
Department of Geriatrics Center, The Fourth People's Hospital of Shenyang, Shenyang, Liaoning, China.
Front Neurol. 2024 Jan 8;14:1303434. doi: 10.3389/fneur.2023.1303434. eCollection 2023.
Parkinson's disease (PD) is the second most common neurodegenerative disease after Alzheimer's disease. Myasthenia gravis (MG) is a rare autoimmune disease caused by antibodies against the neuromuscular junction. PD and comorbid MG are rarely seen.
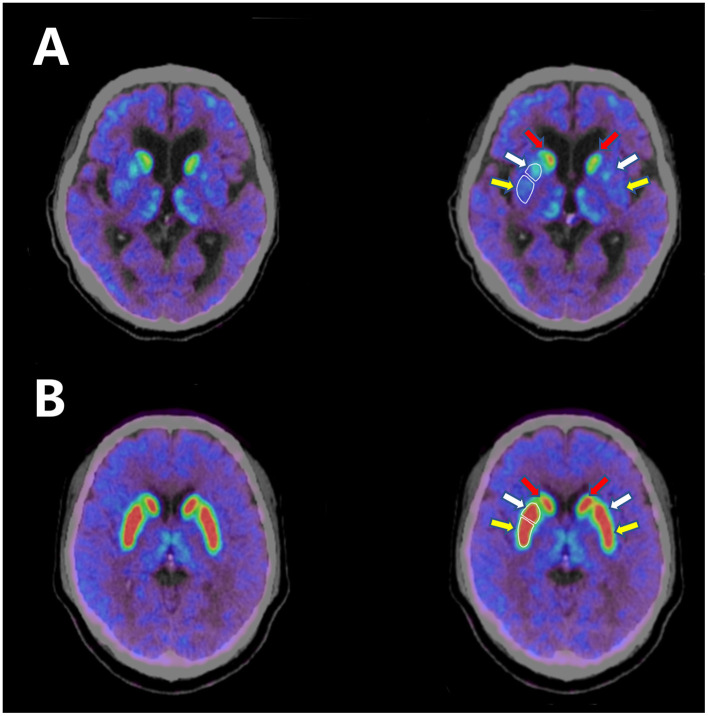
Here we report on a patient who was diagnosed with PD and MG. A 74-year-old man had a 4-year history of bradykinesia and was diagnosed with PD. He subsequently developed incomplete palpebral ptosis, apparent dropped head, and shuffling of gait. The results of neostigmine tests were positive. Repetitive nerve stimulation (RNS) showed significant decremental responses at 3 and 5 Hz in the orbicularis oculi. The patient's anti-acetylcholine receptor (anti-AchR) antibody serum level was also elevated. Meanwhile, 9-[F]fluoropropyl-(+)-dihydrotetrabenazine positron emission tomography-computed tomography (F-AV133 PET-CT) scan revealed a significant decrease in uptake in the bilateral putamen. After addition of cholinesterase inhibitors, his symptoms of palpebral ptosis and head drop improved greatly and he showed a good response to levodopa.
Although PD with MG is rare, we still need to notice the possibility that a PD patient may have comorbid MG. The underlying mechanism of PD and comorbid MG remains unknown, but an imbalance between the neurotransmitters dopamine and acetylcholine and the immune system are likely to play significant roles in the pathogenesis. In this article, we present our case and a literature review on the co-occurrence of PD and MG, reviewing their clinical features, and discuss the underlying pathogenic mechanism of this comorbidity.
帕金森病(PD)是仅次于阿尔茨海默病的第二常见神经退行性疾病。重症肌无力(MG)是一种由抗神经肌肉接头抗体引起的罕见自身免疫性疾病。PD合并MG的情况很少见。
在此我们报告一例被诊断为PD和MG的患者。一名74岁男性有4年运动迟缓病史,被诊断为PD。随后他出现不完全性睑下垂、明显的低头和步态拖曳。新斯的明试验结果为阳性。重复神经电刺激(RNS)显示眼轮匝肌在3Hz和5Hz时出现明显递减反应。患者的抗乙酰胆碱受体(抗AchR)抗体血清水平也升高。同时,9-[F]氟丙基-(+)-二氢四苯嗪正电子发射断层扫描-计算机断层扫描(F-AV133 PET-CT)显示双侧壳核摄取显著降低。加用胆碱酯酶抑制剂后,他的睑下垂和低头症状明显改善,并且对左旋多巴反应良好。
虽然PD合并MG很少见,但我们仍需注意PD患者可能合并MG的可能性。PD合并MG的潜在机制尚不清楚,但神经递质多巴胺和乙酰胆碱之间的失衡以及免疫系统可能在发病机制中起重要作用。在本文中,我们展示了我们的病例以及关于PD和MG共病的文献综述,回顾了它们的临床特征,并讨论了这种共病的潜在致病机制。