School of Architecture and Urban Planning, Chongqing University, Chongqing, China.
Key Laboratory of New Technology for Construction of Cities in Mountain Area, Chongqing University, Chongqing, China.
Front Public Health. 2024 Jan 8;11:1257093. doi: 10.3389/fpubh.2023.1257093. eCollection 2023.
Empirical evidence has shown that light therapy (LT) can reduce depression symptoms by stimulating circadian rhythms. However, there is skepticism and inconclusive results, along with confusion regarding dosing. The purpose of this study is to quantify light as a stimulus for the circadian system and create a dose-response relationship that can help reduce maladies among adolescents and young adults (AYAs). This will provide a reference for light exposure and neural response, which are crucial in the neuropsychological mechanism of light intervention. The study also aims to provide guidance for clinical application.
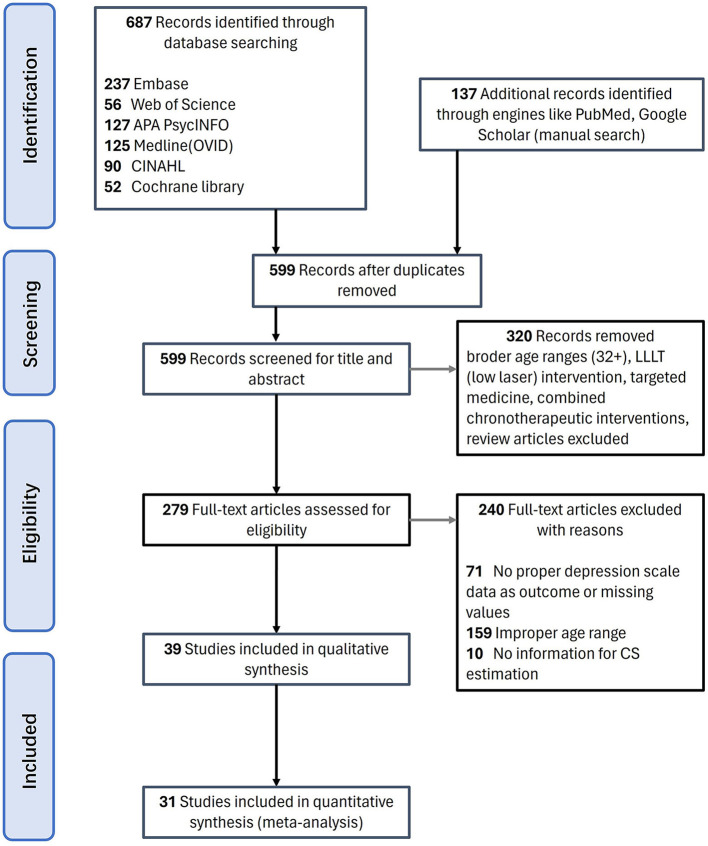
The latest quantitative model of CL (circadian light) and CS (circadian stimulus) was adopted to quantify light dose for circadian phototransduction in youth depression-related light therapy. Articles published up to 2023 through Web of Science, Cochrane Library, Medline (OVID), CINAHL, APA PsycINFO, Embase, and Scholars were retrieved. A meta-analysis of 31 articles (1,031 subjects) was performed using Stata17.0, CMA3.0 (comprehensive meta-analysis version 3.0) software, and Python 3.9 platform for light therapy efficacy comparison and dose-response quantification.
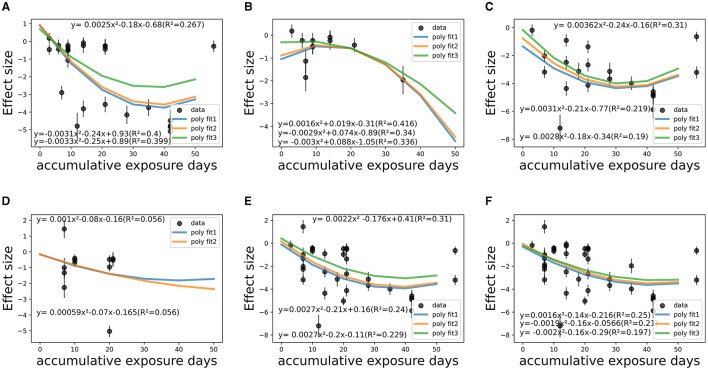
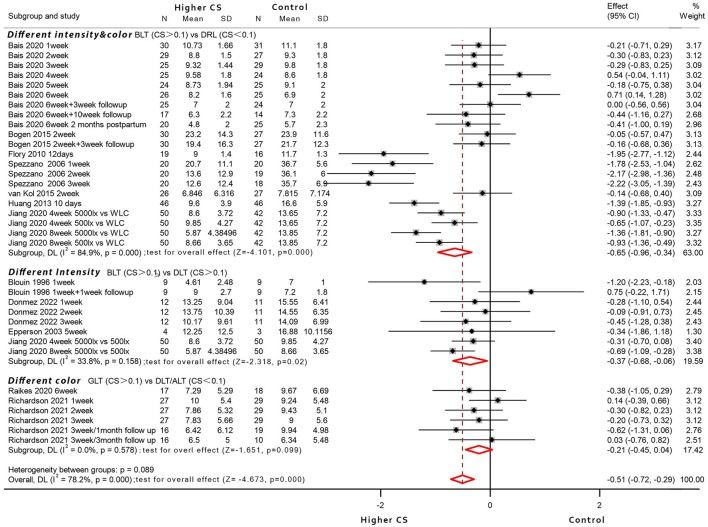
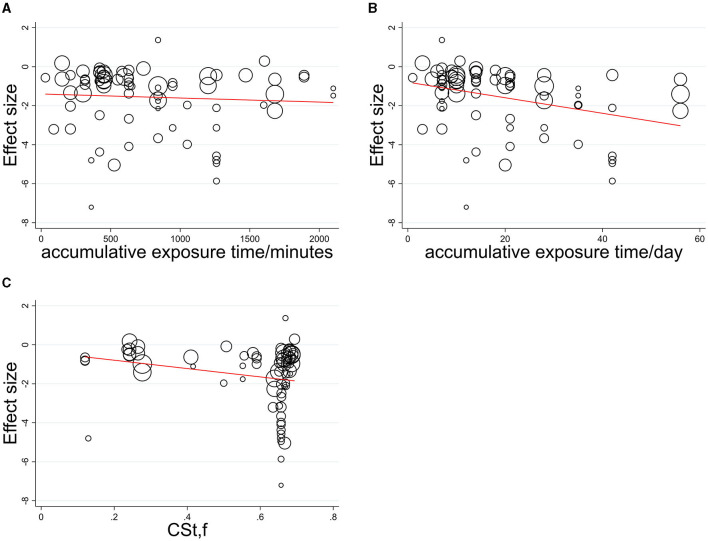
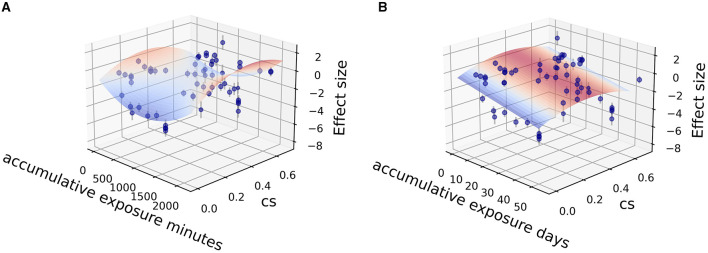
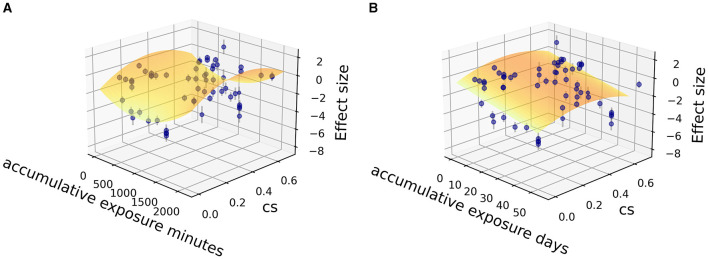
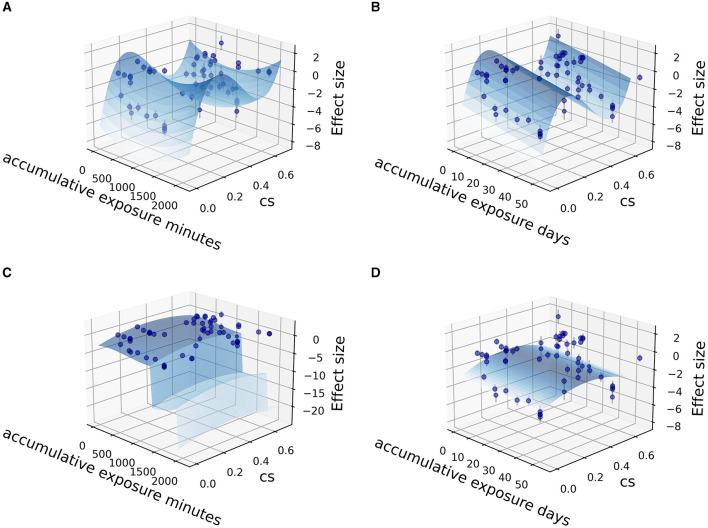
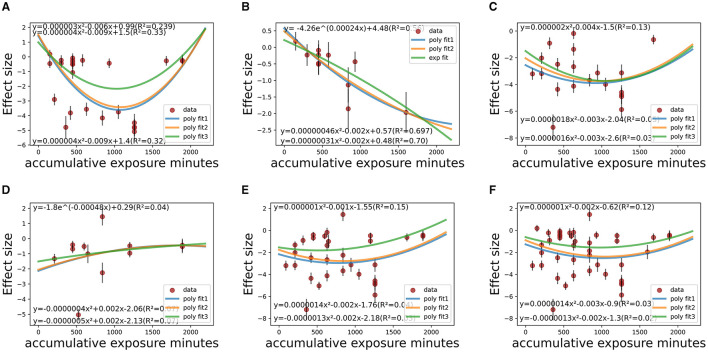
Under various circadian stimulus conditions (0.1 < CS < 0.7) of light therapy (LT), malady reductions among AYAs were observed (pooled SMD = -1.59, 95%CI = -1.86 to -1.32; = -11.654, = 0.000; = 92.8%), with temporal pattern ( = 0.044) and co-medication ( = 0.000) suggested as main heterogeneity sources. For the efficacy advantage of LT with a higher circadian stimulus that is assumed to be influenced by visualization, co-medication, disease severity, and time pattern, sets of meta-analysis among random-controlled trials (RCTs) found evidence for significant efficacy of circadian-active bright light therapy (BLT) over circadian-inactive dim red light (SMD = -0.65, 95% CI = -0.96 to -0.34; = -4.101, = 0.000; = 84.9%) or circadian-active dimmer white light (SMD = -0.37, 95% CI = -0.68 to -0.06; = -2.318, = 0.02; = 33.8%), whereas green-blue, circadian-active BLT showed no significant superiority over circadian-inactive red/amber light controls (SMD = -0.21, 95% CI = -0.45 to 0.04; = -2.318, = 0.099; = 0%). Overall, circadian-active BLT showed a greater likelihood of clinical response than dim light controls, with increased superiority observed with co-medication. For pre-to-post-treatment amelioration and corresponding dose-response relationship, cumulative duration was found more influential than other categorical (co-medication, severity, study design) or continuous (CS) variables. Dose-response fitting indicated that the therapeutic effect would reach saturation among co-medicated patients at 32-42 days (900-1,000 min) and 58-59 days (1,100-1,500 min) among non-medicated AYAs. When exerting high circadian stimulus of light therapy (0.6 < CS < 0.7), there was a significantly greater effect size in 1,000-1,500 min of accumulative duration than <1,000 or >1,500 min of duration, indicating a threshold for practical guidance.
The results have been based on limited samples and influenced by a small sample effect. The placebo effect could not be ignored.
Although the superiority of LT with higher circadian stimulus over dimmer light controls remains unproven, greater response potentials of circadian-active BLT have been noticed among AYAs, taking co-medication, disease severity, time pattern, and visual characteristics into consideration. The dose-response relationship with quantified circadian stimulus and temporal pattern had been elaborated under various conditions to support clinical depression treatment and LT device application in the post-pandemic era.
实证证据表明,光疗(LT)可以通过刺激昼夜节律来减轻抑郁症状。然而,对于剂量存在怀疑和不确定的结果,以及混淆。本研究的目的是量化光作为昼夜系统的刺激因素,并建立剂量-反应关系,以帮助减少青少年和年轻人(AYAs)的疾病。这将为光暴露和神经反应提供参考,这在光干预的神经心理学机制中至关重要。该研究还旨在为临床应用提供指导。
采用最新的 CL(circadian light)和 CS(circadian stimulus)定量模型,对与青少年抑郁相关的光疗中的光治疗昼夜光转导进行光剂量量化。通过 Web of Science、Cochrane Library、Medline(OVID)、CINAHL、APA PsycINFO、Embase 和 Scholars 检索了截至 2023 年的文章。使用 Stata17.0、CMA3.0(综合荟萃分析版本 3.0)软件和 Python 3.9 平台对 31 篇文章(1031 名受试者)进行了荟萃分析,以比较光疗疗效并量化剂量-反应。
在各种昼夜刺激条件(0.1<CS<0.7)下,AYAs 的疾病减轻情况(pooled SMD=-1.59,95%CI=-1.86 至-1.32;= -11.654,= 0.000;= 92.8%),存在时间模式(=0.044)和合并用药(=0.000)作为主要异质性来源。对于假设受可视化、合并用药、疾病严重程度和时间模式影响的昼夜刺激较高的光疗疗效优势,随机对照试验(RCT)的荟萃分析结果表明,昼夜活性强光疗(BLT)对昼夜非活性弱红光(SMD=-0.65,95%CI=-0.96 至-0.34;= -4.101,= 0.000;= 84.9%)或昼夜活性弱白光(SMD=-0.37,95%CI=-0.68 至-0.06;= -2.318,= 0.02;= 33.8%)的疗效具有显著优势,而蓝绿色、昼夜活性 BLT 对昼夜非活性红/琥珀光对照(SMD=-0.21,95%CI=-0.45 至-0.04;= -2.318,= 0.099;= 0%)没有显著优势。总体而言,昼夜活性 BLT 比弱光对照更有可能产生临床反应,并且合并用药的效果更大。对于治疗前后的改善和相应的剂量-反应关系,累积时间比其他类别(合并用药、严重程度、研究设计)或连续(CS)变量更有影响力。剂量反应拟合表明,在合并用药患者中,治疗效果将在 32-42 天(900-1000 分钟)和 58-59 天(1100-1500 分钟)达到饱和,而非合并用药的 AYAs 中则在 1000-1500 分钟累积时间内达到饱和。当发挥较高的昼夜刺激光疗(0.6<CS<0.7)时,在 1000-1500 分钟的累积时间内,光疗的效果大小明显大于<1000 分钟或>1500 分钟的时间,这表明存在实际指导的阈值。
结果基于有限的样本,受小样本效应的影响。安慰剂效应不容忽视。
尽管高昼夜刺激光疗相对于弱光对照的优势仍未得到证实,但昼夜活性 BLT 在 AYAs 中表现出更大的反应潜力,同时考虑到合并用药、疾病严重程度、时间模式和视觉特征。在各种条件下,已经详细阐述了与量化昼夜刺激和时间模式相关的剂量-反应关系,以支持抑郁症的临床治疗和光疗设备在后疫情时代的应用。