Wang Carol, Lebedeva Victoria, Yang Jeffy, Anih Joshua, Park Lily J, Paczkowski Freeman, Roshanov Pavel S
Department of Medicine, Western University, London, ON, Canada.
London Health Sciences Centre, London, ON, Canada.
Perioper Med (Lond). 2024 Jan 23;13(1):5. doi: 10.1186/s13741-023-00358-4.
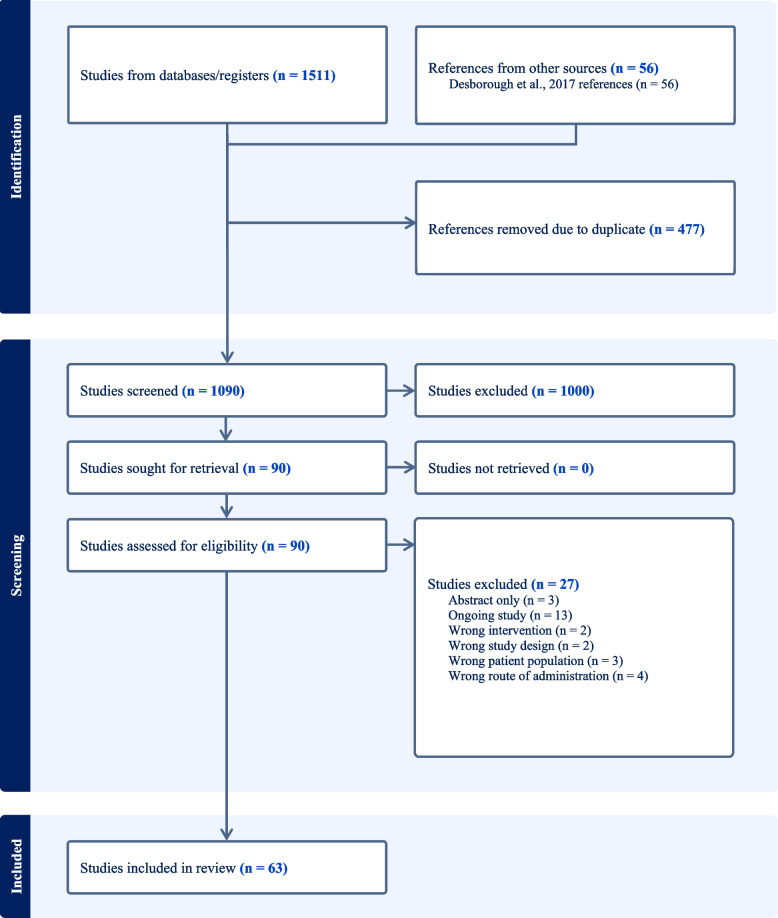
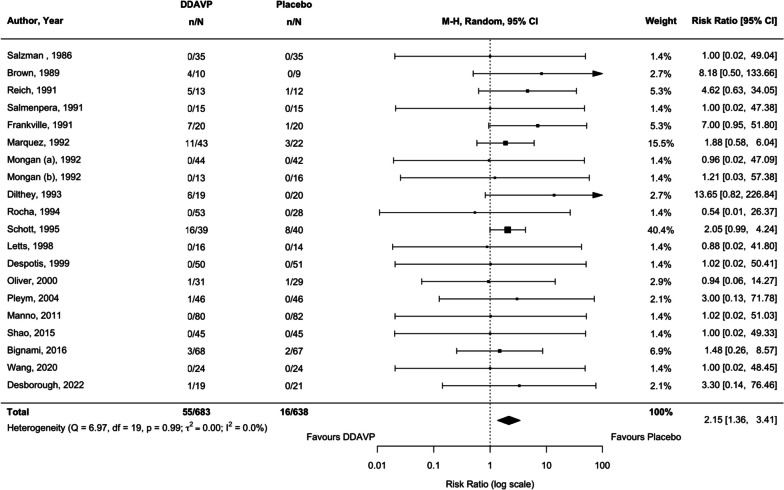
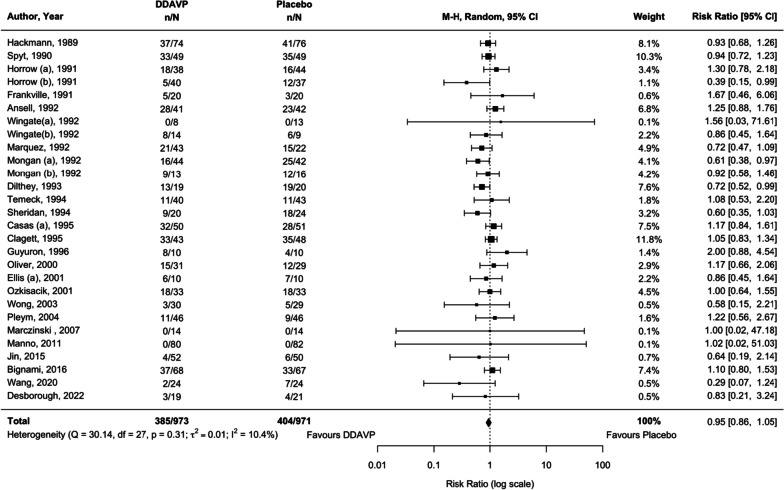
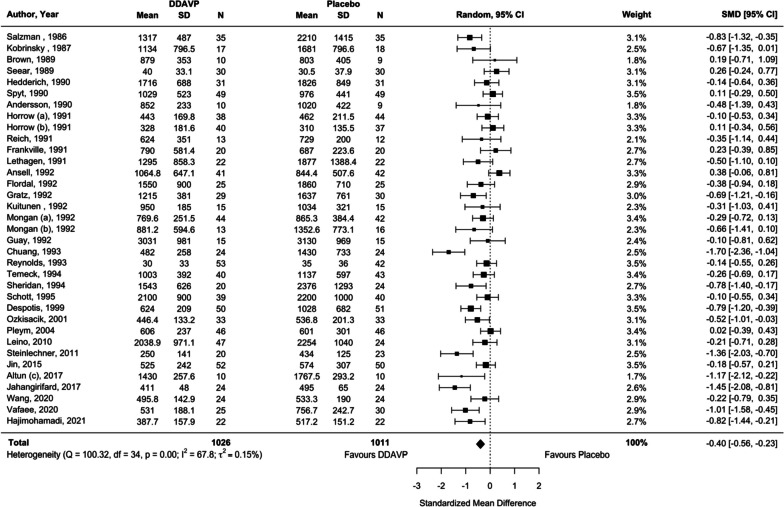
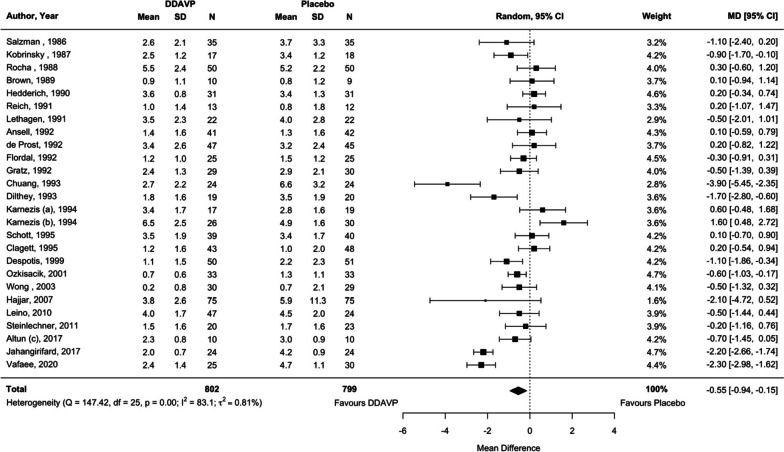
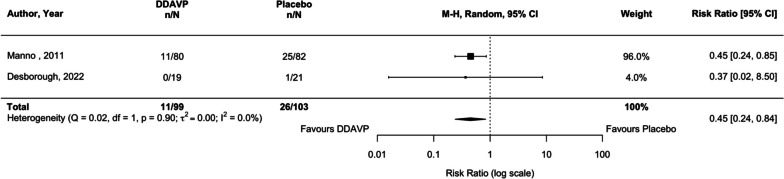
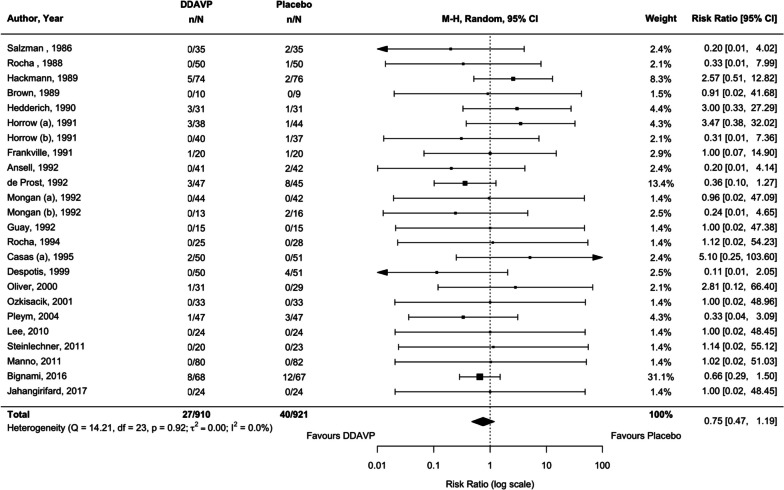
We systematically reviewed the literature to investigate the effects of peri-procedural desmopressin in patients without known inherited bleeding disorders undergoing surgery or other invasive procedures. We included 63 randomized trials (4163 participants) published up to February 1, 2023. Seven trials were published after a 2017 Cochrane systematic review on this topic. There were 38 trials in cardiac surgery, 22 in noncardiac surgery, and 3 in non-surgical procedures. Meta-analyses demonstrated that desmopressin likely does not reduce the risk of receiving a red blood cell transfusion (25 trials, risk ratio [RR] 0.95, 95% confidence interval [CI] 0.86 to 1.05) and may not reduce the risk of reoperation due to bleeding (22 trials, RR 0.75, 95% CI 0.47 to 1.19) when compared to placebo or usual care. However, we demonstrated significant reductions in number of units of red blood cells transfused (25 trials, mean difference -0.55 units, 95% CI - 0.94 to - 0.15), total volume of blood loss (33 trials, standardized mean difference - 0.40 standard deviations; 95% CI - 0.56 to - 0.23), and the risk of bleeding events (2 trials, RR 0.45, 95% CI 0.24 to 0.84). The certainty of evidence of these findings was generally low. Desmopressin increased the risk of clinically significant hypotension that required intervention (19 trials, RR 2.15, 95% CI 1.36 to 3.41). Limited evidence suggests that tranexamic acid is more effective than desmopressin in reducing transfusion risk (3 trials, RR 2.38 favoring tranexamic acid, 95% CI 1.06 to 5.39) and total volume of blood loss (3 trials, mean difference 391.7 mL favoring tranexamic acid, 95% CI - 93.3 to 876.7 mL). No trials directly informed the safety and hemostatic efficacy of desmopressin in advanced kidney disease. In conclusion, desmopressin likely reduces periprocedural blood loss and the number of units of blood transfused in small trials with methodologic limitations. However, the risk of hypotension needs to be mitigated. Large trials should evaluate desmopressin alongside tranexamic acid and enroll patients with advanced kidney disease.
我们系统地回顾了文献,以研究去氨加压素在接受手术或其他侵入性操作、无已知遗传性出血性疾病患者围手术期的作用。我们纳入了截至2023年2月1日发表的63项随机试验(4163名参与者)。7项试验是在2017年Cochrane关于该主题的系统评价之后发表的。其中38项试验涉及心脏手术,22项涉及非心脏手术,3项涉及非手术操作。荟萃分析表明,与安慰剂或常规治疗相比,去氨加压素可能不会降低接受红细胞输血的风险(25项试验,风险比[RR]0.95,95%置信区间[CI]0.86至1.05),也可能不会降低因出血而再次手术的风险(22项试验,RR 0.75,95%CI 0.47至1.19)。然而,我们发现输注红细胞的单位数量显著减少(25项试验,平均差-0.55单位,95%CI -0.94至-0.15),失血总量显著减少(33项试验,标准化平均差-0.40标准差;95%CI -0.56至-0.23),以及出血事件的风险显著降低(2项试验,RR 0.45,95%CI 0.24至0.84)。这些发现的证据确定性普遍较低。去氨加压素增加了需要干预的具有临床意义的低血压风险(19项试验,RR 2.15,95%CI 1.36至3.41)。有限的证据表明,在降低输血风险(3项试验,RR 2.38,支持氨甲环酸,95%CI 1.06至5.39)和失血总量方面(3项试验,平均差391.7mL,支持氨甲环酸,95%CI -93.3至876.7mL),氨甲环酸比去氨加压素更有效。没有试验直接告知去氨加压素在晚期肾病中的安全性和止血效果。总之,在方法学存在局限性的小型试验中,去氨加压素可能会减少围手术期失血和输血单位数量。然而,需要减轻低血压的风险。大型试验应将去氨加压素与氨甲环酸一起评估,并纳入晚期肾病患者。