Anesthesia and Intensive Care, IRCCS Ospedale Policlinico San Martino, Genoa, Italy.
Department of Surgical Science and Integrated Diagnostic, University of Genova, Genoa, Italy.
Intensive Care Med. 2024 Feb;50(2):234-246. doi: 10.1007/s00134-023-07305-3. Epub 2024 Jan 31.
The use of arterial partial pressure of carbon dioxide (PaCO) as a target intervention to manage elevated intracranial pressure (ICP) and its effect on clinical outcomes remain unclear. We aimed to describe targets for PaCO in acute brain injured (ABI) patients and assess the occurrence of abnormal PaCO values during the first week in the intensive care unit (ICU). The secondary aim was to assess the association of PaCO with in-hospital mortality.
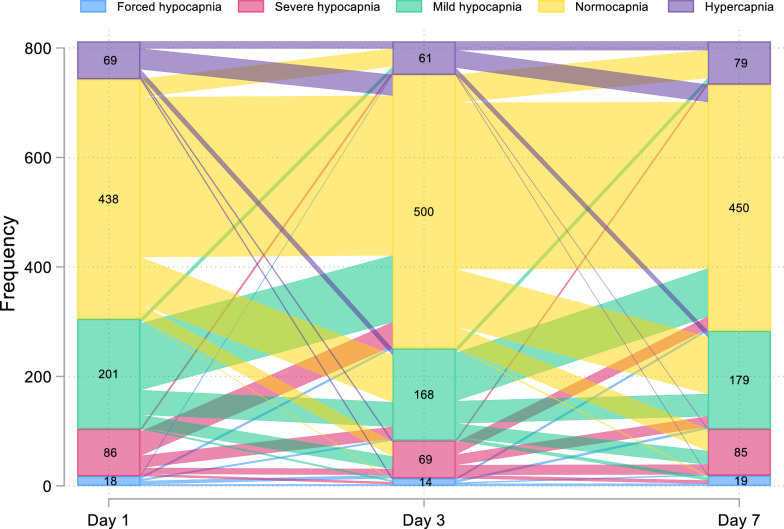
We carried out a secondary analysis of a multicenter prospective observational study involving adult invasively ventilated patients with traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), intracranial hemorrhage (ICH), or ischemic stroke (IS). PaCO was collected on day 1, 3, and 7 from ICU admission. Normocapnia was defined as PaCO > 35 and to 45 mmHg; mild hypocapnia as 32-35 mmHg; severe hypocapnia as 26-31 mmHg, forced hypocapnia as < 26 mmHg, and hypercapnia as > 45 mmHg.
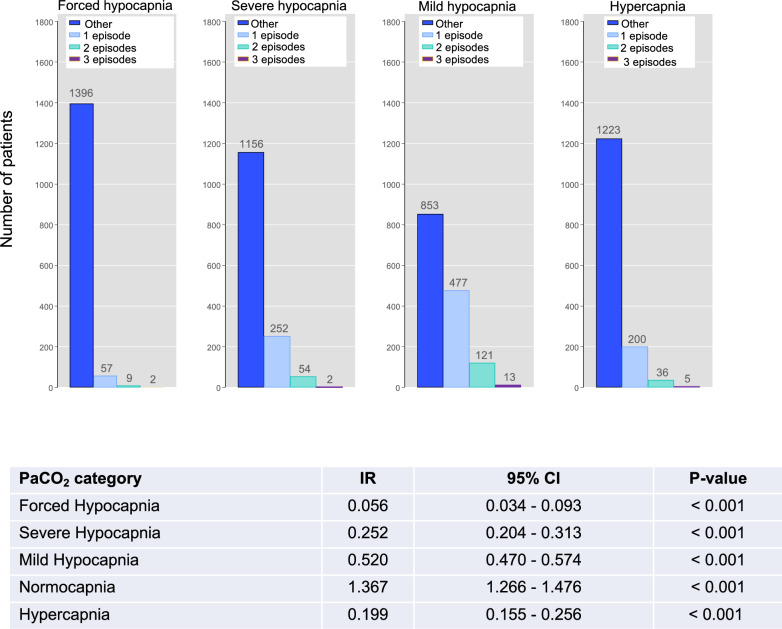
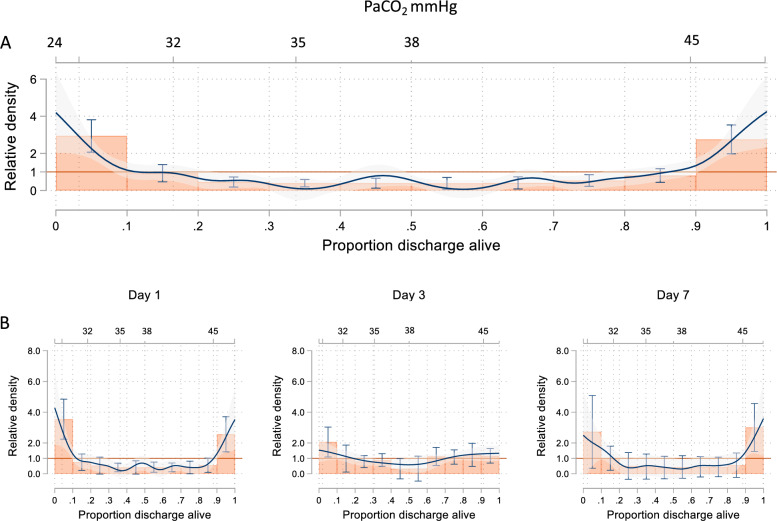
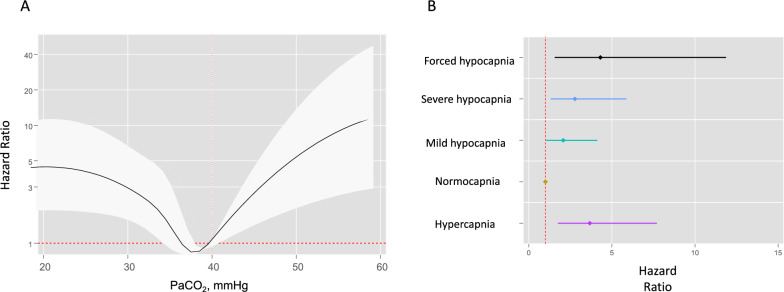
1476 patients (65.9% male, mean age 52 18 years) were included. On ICU admission, 804 (54.5%) patients were normocapnic (incidence 1.37 episodes per person/day during ICU stay), and 125 (8.5%) and 334 (22.6%) were mild or severe hypocapnic (0.52 and 0.25 episodes/day). Forced hypocapnia and hypercapnia were used in 40 (2.7%) and 173 (11.7%) patients. PaCO had a U-shape relationship with in-hospital mortality with only severe hypocapnia and hypercapnia being associated with increased probability of in-hospital mortality (omnibus p value = 0.0009). Important differences were observed across different subgroups of ABI patients.
Normocapnia and mild hypocapnia are common in ABI patients and do not affect patients' outcome. Extreme derangements of PaCO values were significantly associated with increased in-hospital mortality.
动脉血二氧化碳分压(PaCO)作为颅内压(ICP)升高的目标干预手段的使用及其对临床结果的影响仍不清楚。我们旨在描述急性脑损伤(ABI)患者的 PaCO 目标,并评估在 ICU 中第一周内 PaCO 异常值的发生情况。次要目的是评估 PaCO 与院内死亡率的关系。
我们对一项多中心前瞻性观察性研究进行了二次分析,该研究纳入了接受创伤性脑损伤(TBI)、蛛网膜下腔出血(SAH)、颅内出血(ICH)或缺血性卒中(IS)的成年有创通气患者。从 ICU 入院开始,在第 1、3 和 7 天收集 PaCO。正常碳酸血症定义为 PaCO>35 至 45mmHg;轻度低碳酸血症为 32-35mmHg;严重低碳酸血症为 26-31mmHg,强制低碳酸血症为<26mmHg,高碳酸血症为>45mmHg。
共纳入 1476 例患者(65.9%为男性,平均年龄 52 岁±18 岁)。在 ICU 入院时,804 例(54.5%)患者为正常碳酸血症(ICU 住院期间每例患者发生 1.37 次碳酸血症),125 例(8.5%)和 334 例(22.6%)为轻度或严重低碳酸血症(0.52 和 0.25 次/天)。40 例(2.7%)和 173 例(11.7%)患者接受了强制低碳酸血症和高碳酸血症治疗。PaCO 与院内死亡率呈 U 型关系,只有严重低碳酸血症和高碳酸血症与院内死亡率增加相关(总体 p 值=0.0009)。在不同 ABI 患者亚组中观察到显著差异。
正常碳酸血症和轻度低碳酸血症在 ABI 患者中很常见,不会影响患者的预后。PaCO 值的极端变化与院内死亡率的增加显著相关。