Nagashima Koichi, Maruyama Mitsunori, Kaneko Yoshiaki, Sakai Satoshi, Sekihara Takayuki, Kawaji Tetsuma, Iwakawa Hidehiro, Egami Yasuyuki, Ota Chisato, Nagase Satoshi, Yagi Tetsuo, Suzuki Keisuke, Fukaya Hidehira, Nakamura Hironori, Mori Hitoshi, Ueda Akiko, Soejima Kyoko, Watanabe Ryuta, Wakamatsu Yuji, Hirata Shu, Hirata Moyuru, Okumura Yasuo
Division of Cardiology, Department of Medicine Nihon University School of Medicine Tokyo Japan.
Department of Cardiovascular Medicine Nippon Medical School Musashikosugi Hospital Kanagawa Japan.
J Arrhythm. 2023 Dec 15;40(1):131-142. doi: 10.1002/joa3.12976. eCollection 2024 Feb.
This study aimed to establish a systematic method for diagnosing atrioventricular nodal reentrant tachycardia (AVNRT) with a bystander concealed nodoventricular pathway (cNVP).
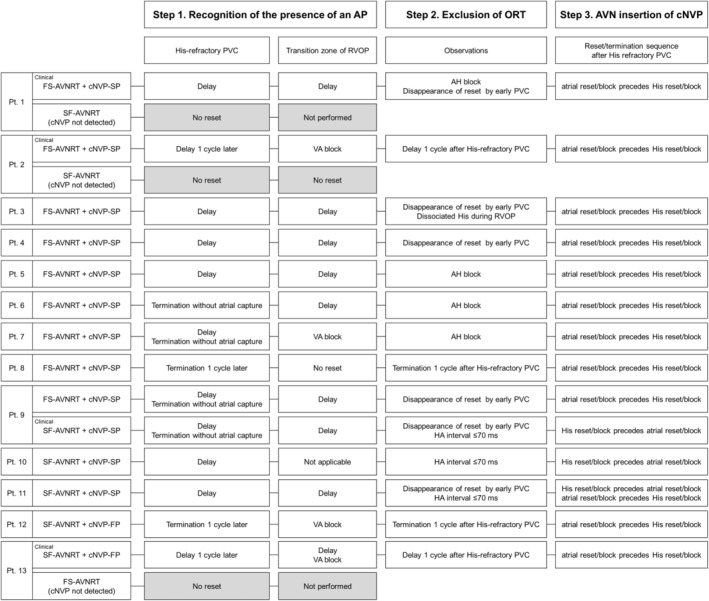
We analyzed 13 cases of AVNRT with a bystander cNVP, 11 connected to the slow pathway (cNVP-SP) and two to the fast pathway (cNVP-FP), along with two cases of cNVP-related orthodromic reciprocating tachycardia (ORT).
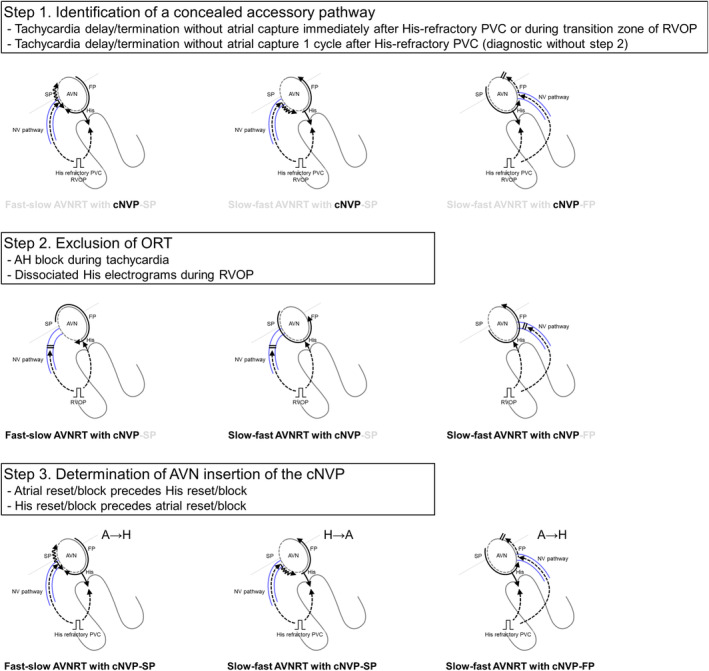
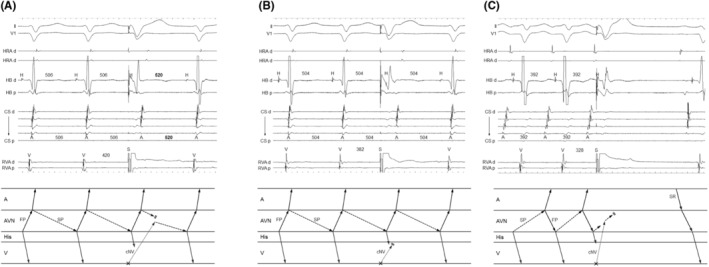
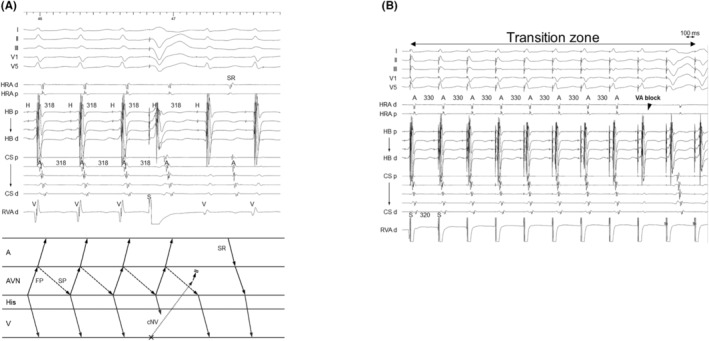
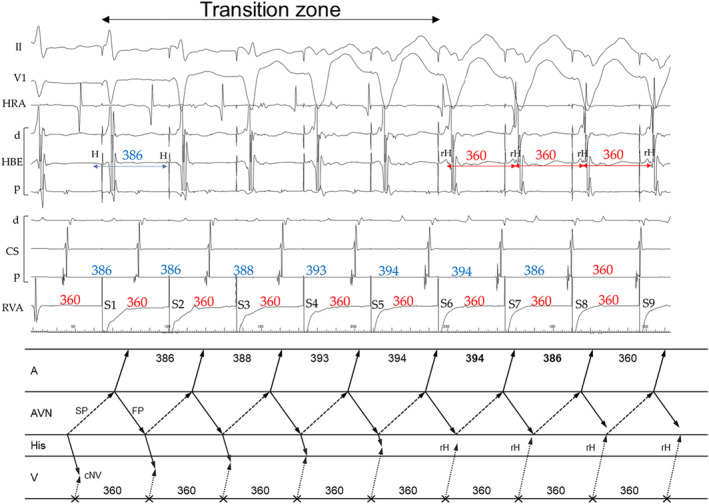
The diagnostic process was summarized in three steps. Step 1 was identification of the presence of an accessory pathway by resetting the tachycardia with delay (n = 9) and termination without atrial capture ( = 4) immediately after delivery of a His-refractory premature ventricular contraction (PVC). Step 2 was exclusion of ORT by atrio-His block during the tachycardia ( = 4), disappearance of the reset phenomenon after the early PVC ( = 7), or dissociation of His from the tachycardia during ventricular overdrive pacing (n = 1). Moreover, tachycardia reset/termination without the atrial capture ( = 2/2) 1 cycle after the His-refractory PVC was specifically diagnostic. Exceptionally, the disappearance of the reset phenomenon was also observed in the two cNVP-ORTs. Step 3 was verification of the AVN as the cNVP insertion site, evidenced by an atrial reset/block preceding the His reset/block in fast-slow AVNRT with a cNVP-SP and slow-fast AVNRT with a cNVP-FP or His reset preceding the atrial reset in slow-fast AVNRT with a cNVP-SP.
AVNRT with a bystander cNVP can be diagnosed in the three steps with few exceptions. Notably, tachycardia reset/termination without atrial capture one cycle after delivery of a His-refractory PVC is specifically diagnostic.
本研究旨在建立一种系统方法,用于诊断伴有旁观者隐匿性结室旁路(cNVP)的房室结折返性心动过速(AVNRT)。
我们分析了13例伴有旁观者cNVP的AVNRT患者,其中11例连接至慢径路(cNVP-SP),2例连接至快径路(cNVP-FP),以及2例与cNVP相关的顺向性折返性心动过速(ORT)。
诊断过程总结为三个步骤。第一步是通过在发放希氏束不应期室性早搏(PVC)后立即延迟重整心动过速(n = 9)和无心房夺获终止心动过速(n = 4)来识别旁路的存在。第二步是通过心动过速期间的房室希氏束阻滞(n = 4)、早期PVC后重整现象消失(n = 7)或心室超速起搏期间希氏束与心动过速分离(n = 1)来排除ORT。此外,希氏束不应期PVC后1个心动周期无心房夺获的心动过速重整/终止具有特异性诊断价值。例外的是,在2例cNVP-ORT中也观察到重整现象消失。第三步是验证房室结为cNVP插入部位,在伴有cNVP-SP的快慢型AVNRT和伴有cNVP-FP的慢快型AVNRT中,希氏束重整/阻滞之前出现心房重整/阻滞,或在伴有cNVP-SP的慢快型AVNRT中希氏束重整先于心房重整,均可证明。
伴有旁观者cNVP的AVNRT可通过这三个步骤进行诊断,例外情况很少。值得注意的是,希氏束不应期PVC后1个心动周期无心房夺获的心动过速重整/终止具有特异性诊断价值。