Siepen Bernhard M, Forfang Elisabeth, Branca Mattia, Drop Boudewijn, Mueller Madlaine, Goeldlin Martina B, Katan Mira, Michel Patrik, Cereda Carlo, Medlin Friedrich, Peters Nils, Renaud Susanne, Niederhauser Julien, Carrera Emmanuel, Kahles Timo, Kägi Georg, Bolognese Manuel, Salmen Stephan, Mono Marie-Luise, Polymeris Alexandros A, Wegener Susanne, Z'Graggen Werner, Kaesmacher Johannes, Schaerer Michael, Rodic Biljana, Kristoffersen Espen Saxhaug, Larsen Kristin T, Wyller Torgeir Bruun, Volbers Bastian, Meinel Thomas R, Arnold Marcel, Engelter Stefan T, Bonati Leo H, Fischer Urs, Rønning Ole Morten, Seiffge David J
Department of Neurology, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Graduate School for Health Sciences, University of Bern, Bern, Switzerland.
Stroke Vasc Neurol. 2024 Dec 30;9(6):640-651. doi: 10.1136/svn-2023-002813.
We investigated outcomes in patients with intracerebral haemorrhage (ICH) according to prior anticoagulation treatment with Vitamin K antagonists (VKAs), direct oral anticoagulants (DOACs) or no anticoagulation.
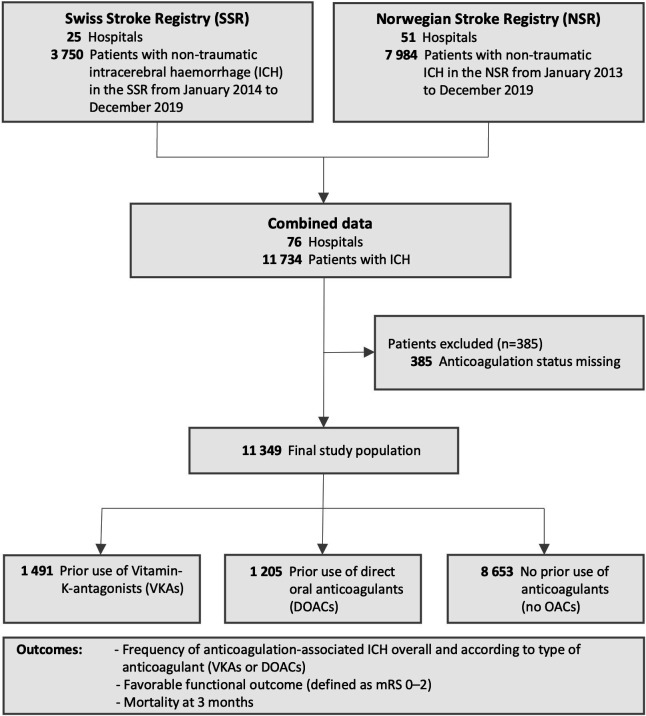
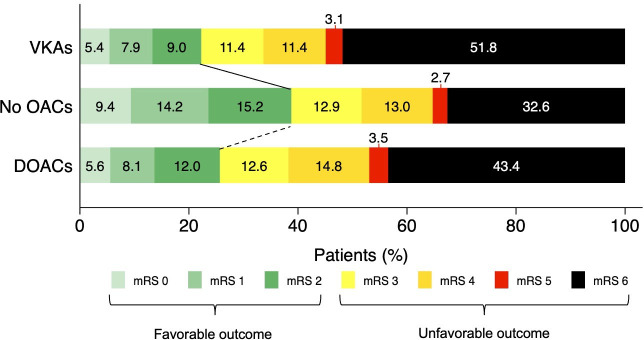
This is an individual patient data study combining two prospective national stroke registries from Switzerland and Norway (2013-2019). We included all consecutive patients with ICH from both registries. The main outcomes were favourable functional outcome (modified Rankin Scale 0-2) and mortality at 3 months.
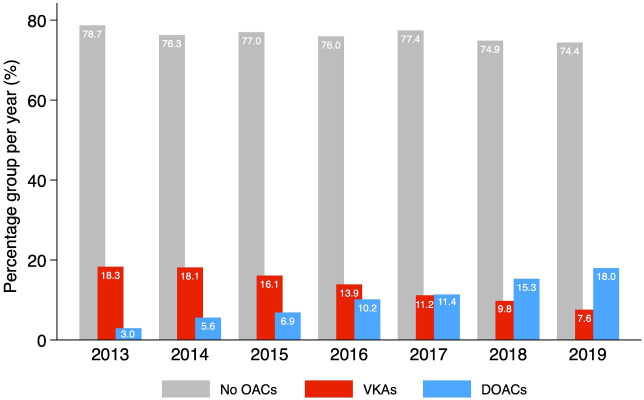
Among 11 349 patients with ICH (mean age 73.6 years; 47.6% women), 1491 (13.1%) were taking VKAs and 1205 (10.6%) DOACs (95.2% factor Xa inhibitors). The median percentage of patients on prior anticoagulation was 23.7 (IQR 22.6-25.1) with VKAs decreasing (from 18.3% to 7.6%) and DOACs increasing (from 3.0% to 18.0%) over time. Prior VKA therapy (n=209 (22.3%); adjusted ORs (aOR), 0.64; 95% CI, 0.49 to 0.84) and prior DOAC therapy (n=184 (25.7%); aOR, 0.64; 95% CI, 0.47 to 0.87) were independently associated with lower odds of favourable outcome compared with patients without anticoagulation (n=2037 (38.8%)). Prior VKA therapy (n=720 (49.4%); aOR, 1.71; 95% CI, 1.41 to 2.08) and prior DOAC therapy (n=460 (39.7%); aOR, 1.28; 95% CI, 1.02 to 1.60) were independently associated with higher odds of mortality compared with patients without anticoagulation (n=2512 (30.2%)).
The spectrum of anticoagulation-associated ICH changed over time. Compared with patients without prior anticoagulation, prior VKA treatment and prior DOAC treatment were independently associated with lower odds of favourable outcome and higher odds of mortality at 3 months. Specific reversal agents unavailable during the study period might improve outcomes of DOAC-associated ICH in the future.
我们根据既往使用维生素K拮抗剂(VKA)、直接口服抗凝剂(DOAC)或未进行抗凝治疗,对脑出血(ICH)患者的预后进行了调查。
这是一项个体患者数据研究,合并了来自瑞士和挪威的两个前瞻性国家卒中登记处(2013 - 2019年)的数据。我们纳入了两个登记处所有连续的ICH患者。主要结局为良好的功能预后(改良Rankin量表评分0 - 2分)和3个月时的死亡率。
在11349例ICH患者中(平均年龄73.6岁;47.6%为女性),1491例(13.1%)正在服用VKA,1205例(10.6%)正在服用DOAC(95.2%为Xa因子抑制剂)。既往接受抗凝治疗患者的中位数百分比为23.7(四分位间距22.6 - 25.1),随着时间推移,VKA使用者比例下降(从18.3%降至7.6%),DOAC使用者比例上升(从3.0%升至18.0%)。与未接受抗凝治疗的患者(n = 2037例(38.8%))相比,既往VKA治疗(n = 209例(22.3%);校正比值比(aOR),0.64;95%置信区间,0.49至0.84)和既往DOAC治疗(n = 184例(25.7%);aOR,0.64;95%置信区间,0.47至0.87)与良好预后的较低几率独立相关。与未接受抗凝治疗的患者(n = 2512例(30.2%))相比,既往VKA治疗(n = 720例(49.4%);aOR,1.71;95%置信区间,1.41至2.08)和既往DOAC治疗(n = 460例(39.7%);aOR,1.28;95%置信区间,1.02至1.60)与较高的死亡几率独立相关。
抗凝相关脑出血的情况随时间发生了变化。与既往未接受抗凝治疗的患者相比,既往VKA治疗和既往DOAC治疗与3个月时良好预后的较低几率以及较高的死亡几率独立相关。研究期间无法获得的特定逆转剂可能会改善未来DOAC相关脑出血的预后。