Department of Anesthesiology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou, China.
Department of Anesthesiology, Xiamen Haicang Hospital, Xiamen, China.
Ann Med. 2024 Dec;56(1):2315229. doi: 10.1080/07853890.2024.2315229. Epub 2024 Feb 12.
Many clinical trials have demonstrated the benefits of intraoperative systemic lidocaine administration in major abdominal surgeries. We tested the hypothesis that systemic lidocaine is associated with an enhanced early quality of recovery in patients following laparoscopic colorectal resection.
We randomly allocated 126 patients scheduled for laparoscopic colorectal surgery in a 1:1 ratio to receive either lidocaine (1.5 mg kg bolus over 10 min, followed by continuous infusion at 2 mg kg h until the end of surgery) or identical volumes and rates of saline. The primary outcome was the Quality of Recovery-15 score assessed 24 h after surgery. Secondary outcomes were areas under the pain numeric rating scale curve over time, 48-h morphine consumption, and adverse events.
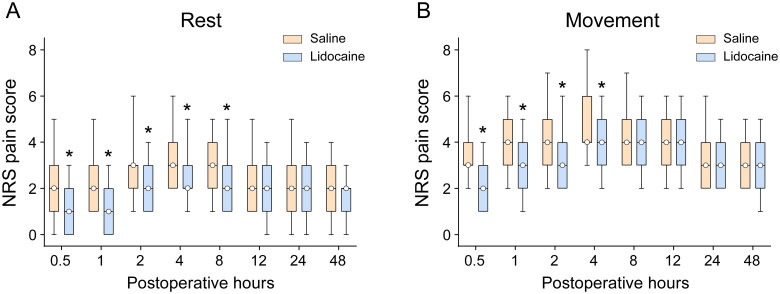
Compared with saline, systemic lidocaine improved the Quality of Recovery-15 score 24 h postoperatively, with a median difference of 4 (95% confidence interval: 1-6; = 0.015). Similarly, the area under the pain numeric rating scale curve over 48 h at rest and on movement was reduced in the lidocaine group ( = 0.004 and < 0.001, respectively). However, these differences were not clinically meaningful. Lidocaine infusion reduced the intraoperative remifentanil requirements but not postoperative 48-h morphine consumption ( < 0.001 and = 0.34, respectively). Additionally, patients receiving lidocaine had a quicker and earlier return of bowel function, as indicated by a shorter time to first flatus (log-rank < 0.001), yet ambulation time was similar between groups (log-rank test, = 0.11).
In patients undergoing laparoscopic colorectal surgery, intraoperative systemic lidocaine resulted in statistically but not clinically significant improvements in quality of recovery (see Graphical Abstract). Chinese Clinical Trial Registry; ChiCTR1900027635.
许多临床试验已经证实,在大型腹部手术中,术中给予全身利多卡因具有益处。我们验证了这样一个假设,即全身给予利多卡因与腹腔镜结直肠切除术后患者早期恢复质量的提高有关。
我们将 126 例择期行腹腔镜结直肠手术的患者按 1:1 的比例随机分配,分别接受利多卡因(1.5mg/kg 于 10min 内推注,随后以 2mg/kg/h 的速度持续输注,直至手术结束)或等容量和等速度的生理盐水。主要结局是术后 24h 时采用恢复质量 15 项评分(Quality of Recovery-15 score)评估。次要结局是疼痛数字评分量表曲线下面积随时间的变化、48h 吗啡用量以及不良事件。
与生理盐水相比,全身给予利多卡因可改善术后 24h 时的恢复质量 15 评分,中位数差值为 4(95%置信区间:1-6;=0.015)。同样,在静息和运动时,48h 内疼痛数字评分量表曲线下面积在利多卡因组也有所减少(分别为=0.004 和<0.001)。然而,这些差异并无临床意义。利多卡因输注减少了术中瑞芬太尼的需求,但并未减少术后 48h 吗啡用量(分别为<0.001 和=0.34)。此外,接受利多卡因治疗的患者更快更早地恢复肠道功能,表现为首次排气时间更短(对数秩检验,<0.001),但两组的下床时间相似(对数秩检验,=0.11)。
在接受腹腔镜结直肠手术的患者中,术中给予全身利多卡因可使恢复质量得到统计学但无临床意义的改善(参见图表摘要)。中国临床试验注册中心;ChiCTR1900027635。