School of Public Health, University of Haifa, Haifa, Israel.
Division of Computational Biology, Mayo Clinic, Rochester, MN.
Blood Adv. 2024 May 14;8(9):2118-2129. doi: 10.1182/bloodadvances.2023012242.
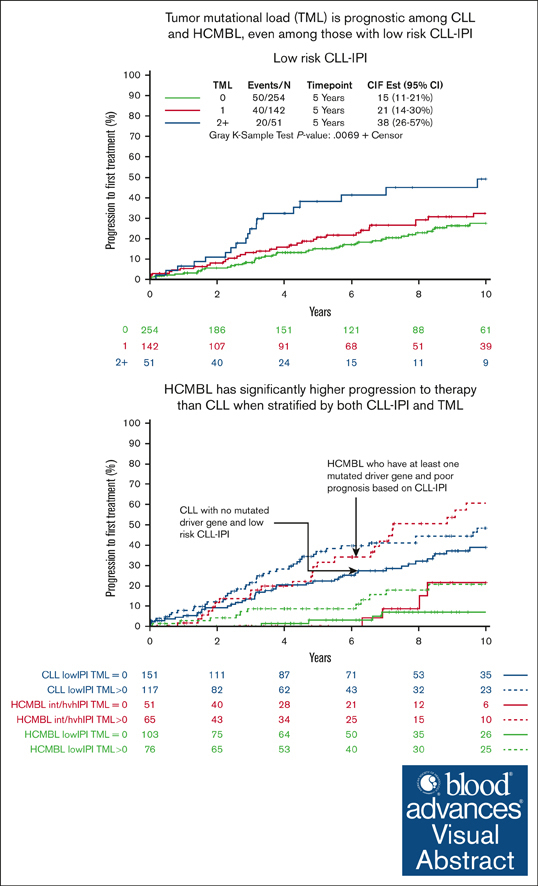
High-count monoclonal B-cell lymphocytosis (HCMBL) is a precursor condition to chronic lymphocytic leukemia (CLL). We have shown that among individuals with HCMBL, the CLL-International Prognostic Index (CLL-IPI) is prognostic for time-to-first therapy (TTFT). Little is known about the prognostic impact of somatically mutated genes among individuals with HCMBL. We sequenced DNA from 371 individuals with HCMBL using a targeted sequencing panel of 59 recurrently mutated genes in CLL to identify high-impact mutations. We compared the sequencing results with that of our treatment-naïve CLL cohort (N = 855) and used Cox regression to estimate hazard ratios and 95% confidence intervals (CIs) for associations with TTFT. The frequencies of any mutated genes were lower in HCMBL (52%) than CLL (70%). At 10 years, 37% of individuals with HCMBL with any mutated gene had progressed requiring treatment compared with 10% among individuals with HCMBL with no mutations; this led to 5.4-fold shorter TTFT (95% CI, 2.6-11.0) among HCMBL with any mutated gene vs none, independent of CLL-IPI. When considering individuals with low risk of progression according to CLL-IPI, those with HCMBL with any mutations had 4.3-fold shorter TTFT (95% CI, 1.6-11.8) vs those with none. Finally, when considering both CLL-IPI and any mutated gene status, we observed individuals with HCMBL who were high risk for both prognostic factors had worse prognosis than patients with low-risk CLL (ie, 5-year progression rate of 32% vs 21%, respectively). Among HCMBL, the frequency of somatically mutated genes at diagnosis is lower than that of CLL. Accounting for both the number of mutated genes and CLL-IPI can identify individuals with HCMBL with more aggressive clinical course.
高计数单克隆 B 细胞淋巴增生症 (HCMBL) 是慢性淋巴细胞白血病 (CLL) 的前体状态。我们已经表明,在 HCMBL 患者中,CLL-国际预后指数 (CLL-IPI) 可预测首次治疗时间 (TTFT)。关于 HCMBL 患者中体细胞突变基因的预后影响知之甚少。我们使用针对 CLL 中 59 个高频突变基因的靶向测序面板对 371 例 HCMBL 患者的 DNA 进行了测序,以确定高影响突变。我们将测序结果与我们的初治 CLL 队列 (N=855) 进行了比较,并使用 Cox 回归来估计与 TTFT 相关的风险比和 95%置信区间 (CI)。在 HCMBL 中,任何突变基因的频率 (52%) 均低于 CLL (70%)。在 10 年内,37%的 HCMBL 患者有任何突变基因进展需要治疗,而 HCMBL 无突变患者中这一比例为 10%;这导致 HCMBL 中有任何突变基因的 TTFT 缩短了 5.4 倍 (95%CI,2.6-11.0),而 CLL-IPI 则无关。当根据 CLL-IPI 考虑进展风险较低的个体时,HCMBL 中有任何突变的患者 TTFT 缩短了 4.3 倍 (95%CI,1.6-11.8),而无突变的患者 TTFT 则缩短了 4.3 倍。最后,当同时考虑 CLL-IPI 和任何突变基因状态时,我们观察到 HCMBL 中同时具有这两个预后因素高危的患者比低危 CLL 患者预后更差 (即,5 年进展率分别为 32%和 21%)。在 HCMBL 中,诊断时体细胞突变基因的频率低于 CLL。同时考虑突变基因的数量和 CLL-IPI 可以识别出具有更具侵袭性临床病程的 HCMBL 患者。