Cortigiani Lauro, Gaibazzi Nicola, Ciampi Quirino, Rigo Fausto, Rodríguez-Zanella Hugo, Wierzbowska-Drabik Karina, Kasprzak Jaroslaw D, Arbucci Rosina, Lowenstein Jorge, Zagatina Angela, Bartolacelli Ylenia, Gregori Dario, Carerj Scipione, Pepi Mauro, Pellikka Patricia A, Picano Eugenio
Cardiology Division, San Luca Hospital Lucca Italy.
Cardiology Department, Parma University Hospital Parma Italy.
J Am Heart Assoc. 2024 Feb 20;13(4):e031270. doi: 10.1161/JAHA.123.031270. Epub 2024 Feb 16.
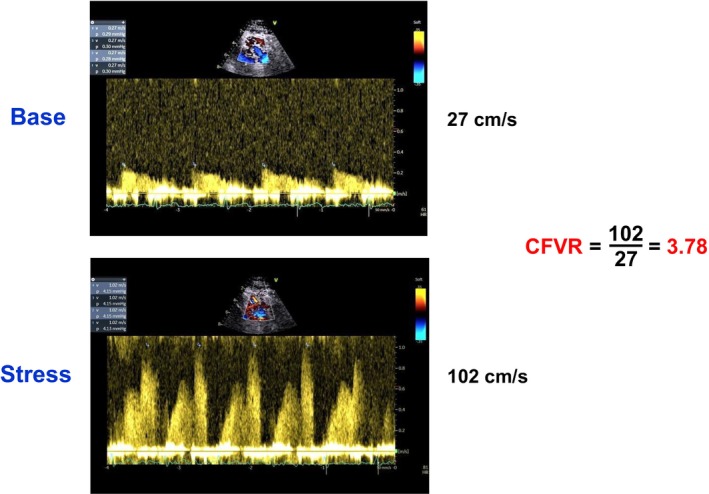
Resting coronary flow velocity (CFV) in the mid-distal left anterior descending coronary artery can be easily assessed with transthoracic echocardiography. In this observational study, the authors sought to assess the relationship between resting CFV, CFV reserve (CFVR), and outcome in patients with chronic coronary syndromes.
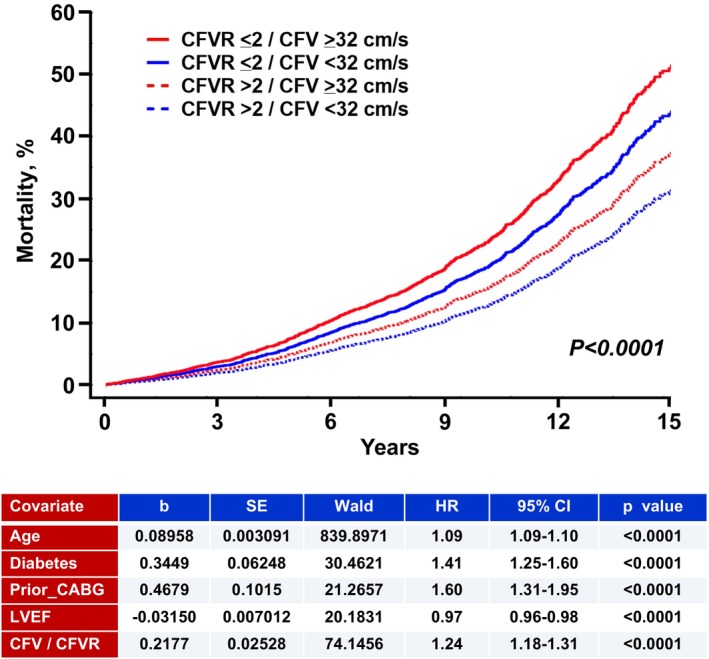
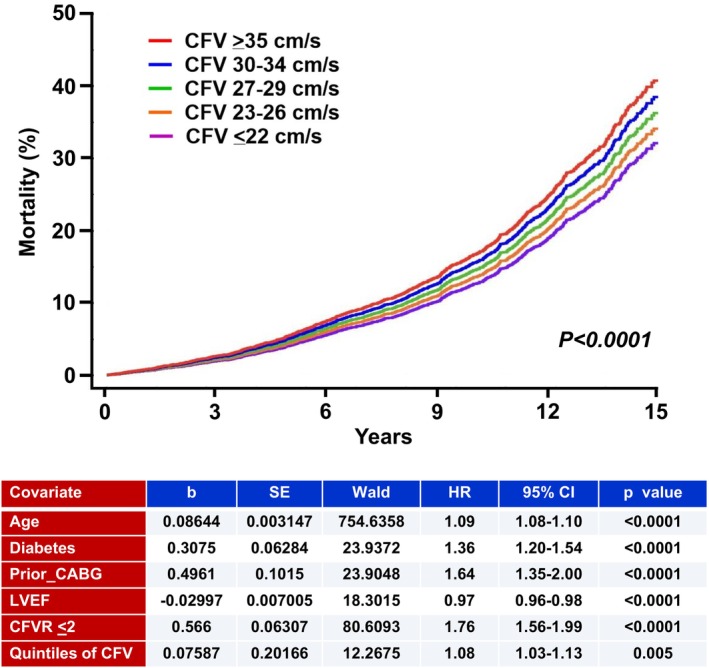
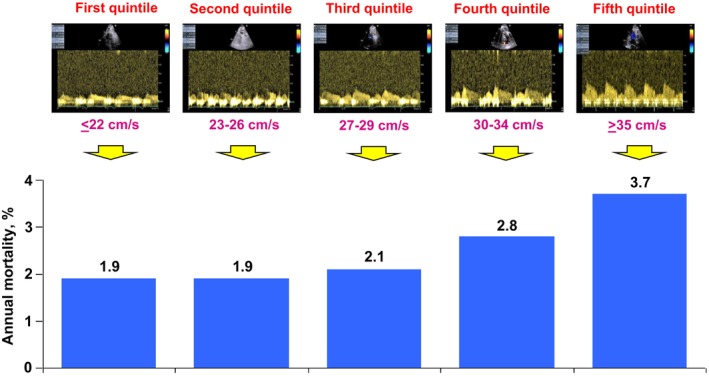
In a prospective multicenter study design, the authors retrospectively analyzed 7576 patients (age, 66±11 years; 4312 men) with chronic coronary syndromes and left ventricular ejection fraction ≥50% referred for dipyridamole stress echocardiography. Recruitment (years 2003-2021) involved 7 accredited laboratories, with interobserver variability <10% for CFV measurement at study entry. Baseline peak diastolic CFV was obtained by pulsed-wave Doppler in the mid-distal left anterior descending coronary artery. CFVR (abnormal value ≤2.0) was assessed with dipyridamole. All-cause death was the only end point. The mean CFV of the left anterior descending coronary artery was 31±12 cm/s. The mean CFVR was 2.32±0.60. During a median follow-up of 5.9±4.3 years, 1121 (15%) patients died. At multivariable analysis, resting CFV ≥32 cm/s was identified by a receiver operating curve as the best cutoff and was independently associated with mortality (hazard ratio [HR], 1.24 [95% CI, 1.10-1.40]; <0.0001) together with CFVR ≤2.0 (HR, 1.78 [95% CI, 1.57-2.02]; <0.0001), age, diabetes, history of coronary surgery, and left ventricular ejection fraction. When both CFV and CFVR were considered, the mortality rate was highest in patients with resting CFV ≥32 cm/s and CFVR ≤2.0 and lowest in patients with resting CFV <32 cm/s and CFVR >2.0.
High resting CFV is associated with worse survival in patients with chronic coronary syndromes and left ventricular ejection fraction ≥50%. The value is independent and additive to CFVR. The combination of high resting CFV and low CFVR is associated with the worst survival.
经胸超声心动图可轻松评估左前降支冠状动脉中远端的静息冠状动脉血流速度(CFV)。在这项观察性研究中,作者试图评估慢性冠状动脉综合征患者的静息CFV、CFV储备(CFVR)与预后之间的关系。
在一项前瞻性多中心研究设计中,作者回顾性分析了7576例慢性冠状动脉综合征且左心室射血分数≥50%的患者(年龄66±11岁;4312例男性),这些患者因双嘧达莫负荷超声心动图检查前来就诊。招募工作(2003年至2021年)涉及7个认可的实验室,研究开始时CFV测量的观察者间变异性<10%。通过脉冲波多普勒在左前降支冠状动脉中远端获取基线舒张期峰值CFV。使用双嘧达莫评估CFVR(异常值≤2.0)。全因死亡是唯一的终点。左前降支冠状动脉的平均CFV为31±12 cm/s。平均CFVR为2.32±0.60。在中位随访5.9±4.3年期间,1121例(15%)患者死亡。在多变量分析中,通过受试者工作特征曲线确定静息CFV≥32 cm/s为最佳截断值,其与死亡率独立相关(风险比[HR],1.24[95%CI,1.10 - 1.40];P<0.0001),CFVR≤2.0(HR,1.78[95%CI, 1.57 - 2.02];P<0.0001)、年龄、糖尿病、冠状动脉手术史和左心室射血分数也与死亡率独立相关。当同时考虑CFV和CFVR时,静息CFV≥32 cm/s且CFVR≤2.0的患者死亡率最高,静息CFV<32 cm/s且CFVR>2.0的患者死亡率最低。
在慢性冠状动脉综合征且左心室射血分数≥50%的患者中,高静息CFV与较差的生存率相关。该指标独立于CFVR且具有相加作用。高静息CFV和低CFVR的组合与最差的生存率相关。