Amikam Uri, Badeghiesh Ahmad, Baghlaf Haitham, Brown Richard, Dahan Michael H
Department of Obstetrics and Gynecology, McGill University, Montréal, Quebec, Canada.
The Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Heliyon. 2024 Feb 6;10(4):e25631. doi: 10.1016/j.heliyon.2024.e25631. eCollection 2024 Feb 29.
Cerebrovascular accidents (CVA) in childbearing-age women are rare. We aimed to evaluate the association between CVA events prior to delivery and obstetrical and neonatal outcomes.
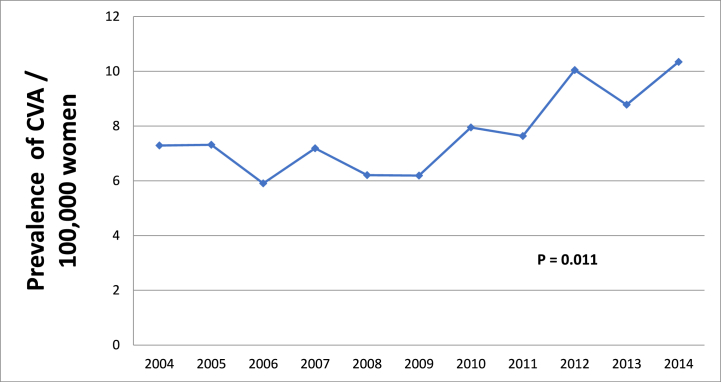
A retrospective cohort study was conducted using data from the Healthcare Cost and Utilization Project, Nationwide Inpatient Sample (HCUP-NIS) database. All pregnant women who delivered or had a maternal death in the US from 2004 to 2014 were included in the study. We performed a comparison between women with an ICD-9 diagnosis of CVA before the delivery admission and those without. Obstetrical and neonatal outcomes were compared between the two groups.
In total, 9,096,788 women fulfilled the inclusion criteria. Among them, 695 women (7.6 per 100,000) were diagnosed with a CVA before delivery. Women with a history of CVA, compared to those without, were more likely to be Black, older than 35 years of age, and suffer from obesity, chronic hypertension, pregestational diabetes, and thyroid disease. Patients with a prior CVA, compared to those without, had higher rates of pregnancy-induced hypertension (aOR 6.41, 95% CI 5.03-8.39, p < 0.001), preeclampsia (aOR 7.65, 95% CI 6.03-9.71, p < 0.001), and eclampsia (aOR 171.56, 95% CI 124.63-236.15, p < 0.001). Additionally, they had higher rates of preterm delivery (aOR 1.72, 95% CI 1.33-2.22,p = 0.003), cesarean section (aOR 2.69, 95% CI 2.15-3.37, p < 0.001), and maternal complications such as a peripartum hysterectomy (aOR 11.62, 95% CI 5.77-23.41, p < 0.001), postpartum hemorrhage (aOR 3.39, 95 % CI 2.52-4.54, p < 0.001), disseminated intravascular coagulation (aOR 16.32, 95% CI 11.33-23.52, p < 0.001), venous thromboembolism (aOR 45.08, 95% CI 27.17-74.8, p < 0.001), and maternal death (aOR 486.11, 95% CI 307.26-769.07, p < 0.001). Regarding neonatal outcomes, patients with a prior CVA, compared to those without, had a higher rate of intrauterine fetal demise and congenital anomalies.
Women with a CVA event before delivery have a significantly higher incidence of maternal complications, including hypertensive disorders of pregnancy, and neonatal complications, such as intrauterine fetal demise and congenital anomalies. Rates of maternal death were dramatically increased, and this association requires further evaluation.
育龄期妇女脑血管意外(CVA)较为罕见。我们旨在评估分娩前发生CVA事件与产科及新生儿结局之间的关联。
利用医疗成本与利用项目全国住院样本(HCUP-NIS)数据库中的数据进行一项回顾性队列研究。纳入2004年至2014年在美国分娩或发生孕产妇死亡的所有孕妇。我们对分娩入院前诊断为CVA(ICD-9编码)的妇女与未诊断为CVA的妇女进行了比较。比较了两组的产科和新生儿结局。
共有9,096,788名妇女符合纳入标准。其中,695名妇女(每10万人中有7.6人)在分娩前被诊断为CVA。有CVA病史的妇女与无CVA病史的妇女相比,更可能为黑人、年龄超过35岁,且患有肥胖症、慢性高血压、孕前糖尿病和甲状腺疾病。与无CVA病史的患者相比,有CVA病史的患者发生妊娠高血压(调整后比值比[aOR] 6.41,95%置信区间[CI] 5.03 - 8.39,p < 0.001)、先兆子痫(aOR 7.65,95% CI 6.03 - 9.71,p < 0.001)和子痫(aOR 171.56,95% CI 124.63 - 236.15,p < 0.001)的几率更高。此外,她们发生早产(aOR 1.72,95% CI 1.33 - 2.22,p = 0.003)、剖宫产(aOR 2.69,95% CI 2.15 - 3.37,p < 0.001)以及围产期子宫切除术(aOR 11.62,95% CI 5.77 - 23.41,p < 0.001)、产后出血(aOR 3.39,95% CI 2.52 - 4.54,p < 0.001)、弥散性血管内凝血(aOR 16.32,95% CI 11.33 - 23.52,p < 0.001)、静脉血栓栓塞(aOR 45.08,95% CI 27.17 - 74.8,p < 0.001)和孕产妇死亡(aOR 486.11,95% CI 307.26 - 769.07,p < 0.001)等孕产妇并发症的几率更高。关于新生儿结局,有CVA病史的患者与无CVA病史的患者相比,胎儿宫内死亡和先天性异常的发生率更高。
分娩前发生CVA事件的妇女发生包括妊娠高血压疾病在内的孕产妇并发症以及胎儿宫内死亡和先天性异常等新生儿并发症的发生率显著更高。孕产妇死亡率大幅增加,这种关联需要进一步评估。