Wang Hsuan-Yuan, Li Leike, Nelson Cody S, Barfield Richard, Valencia Sarah, Chan Cliburn, Muramatsu Hiromi, Lin Paulo J C, Pardi Norbert, An Zhiqiang, Weissman Drew, Permar Sallie R
Department of Pediatrics, Weill Cornell Medicine, New York, NY, 10065, USA.
Duke University Medical Center, Duke Human Vaccine Institute, Durham, NC, 27710, USA.
NPJ Vaccines. 2024 Feb 20;9(1):38. doi: 10.1038/s41541-024-00821-3.
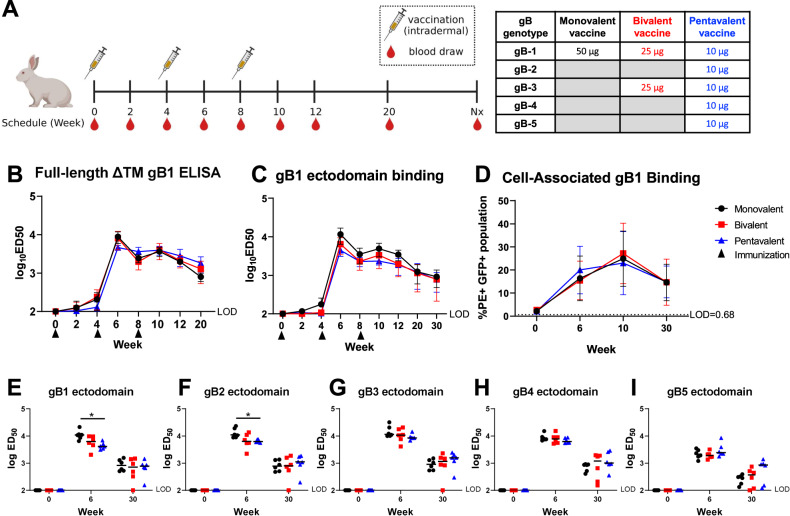
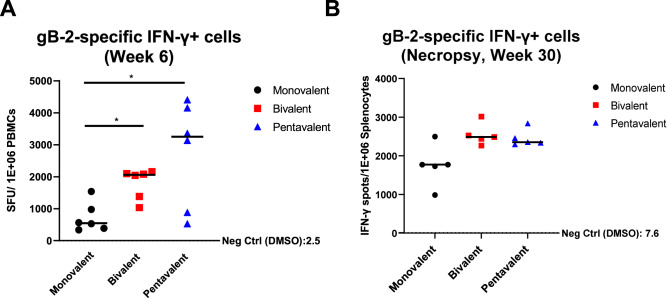
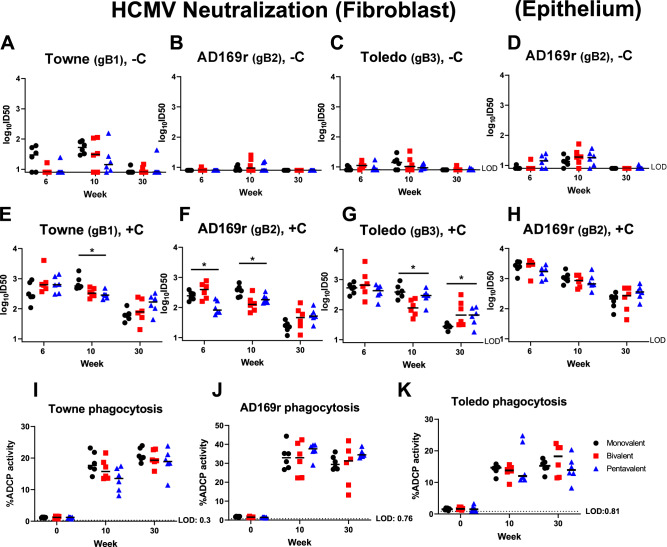
Human cytomegalovirus (HCMV) remains the most common congenital infection and infectious complication in immunocompromised patients. The most successful HCMV vaccine to date, an HCMV glycoprotein B (gB) subunit vaccine adjuvanted with MF59, achieved 50% efficacy against primary HCMV infection. A previous study demonstrated that gB/MF59 vaccinees were less frequently infected with HCMV gB genotype strains most similar to the vaccine strain than strains encoding genetically distinct gB genotypes, suggesting strain-specific immunity accounted for the limited efficacy. To determine whether vaccination with multiple HCMV gB genotypes could increase the breadth of anti-HCMV gB humoral and cellular responses, we immunized 18 female rabbits with monovalent (gB-1), bivalent (gB-1+gB-3), or pentavalent (gB-1+gB-2+gB-3+gB-4+gB-5) gB lipid nanoparticle-encapsulated nucleoside-modified RNA (mRNA-LNP) vaccines. The multivalent vaccine groups did not demonstrate a higher magnitude or breadth of the IgG response to the gB ectodomain or cell-associated gB compared to that of the monovalent vaccine. Also, the multivalent vaccines did not show an increase in the breadth of neutralization activity and antibody-dependent cellular phagocytosis against HCMV strains encoding distinct gB genotypes. Interestingly, peripheral blood mononuclear cell-derived gB-2-specific T-cell responses elicited by multivalent vaccines were of a higher magnitude compared to that of monovalent vaccinated animals against a vaccine-mismatched gB genotype at peak immunogenicity. Yet, no statistical differences were observed in T cell response against gB-3 and gB-5 variable regions among the three vaccine groups. Our data suggests that the inclusion of multivalent gB antigens is not an effective strategy to increase the breadth of anti-HCMV gB antibody and T cell responses. Understanding how to increase the HCMV vaccine protection breadth will be essential to improve the vaccine efficacy.
人巨细胞病毒(HCMV)仍然是免疫功能低下患者中最常见的先天性感染和感染性并发症。迄今为止最成功的HCMV疫苗是一种与MF59佐剂联合使用的HCMV糖蛋白B(gB)亚单位疫苗,对原发性HCMV感染的有效率达到50%。先前的一项研究表明,与编码基因不同的gB基因型的毒株相比,接种gB/MF59疫苗的人感染与疫苗株最相似的HCMV gB基因型毒株的频率较低,这表明毒株特异性免疫是导致疗效有限的原因。为了确定接种多种HCMV gB基因型疫苗是否能增加抗HCMV gB体液和细胞反应的广度,我们用单价(gB-1)、二价(gB-1+gB-3)或五价(gB-1+gB-2+gB-3+gB-4+gB-5)gB脂质纳米颗粒包裹的核苷修饰RNA(mRNA-LNP)疫苗免疫了18只雌性兔子。与单价疫苗组相比,多价疫苗组对gB胞外域或细胞相关gB的IgG反应的强度或广度并没有更高。此外,多价疫苗对编码不同gB基因型的HCMV毒株的中和活性和抗体依赖性细胞吞噬作用的广度也没有增加。有趣的是,在免疫原性峰值时,与单价疫苗接种的动物相比,多价疫苗引发的外周血单核细胞衍生的gB-2特异性T细胞反应针对与疫苗不匹配的gB基因型的强度更高。然而,在三个疫苗组中,针对gB-3和gB-5可变区的T细胞反应没有观察到统计学差异。我们的数据表明,包含多价gB抗原不是增加抗HCMV gB抗体和T细胞反应广度的有效策略。了解如何增加HCMV疫苗的保护广度对于提高疫苗疗效至关重要。