Department of Orthopedics, Peking University Third Hospital, Beijing, China.
Beijing Key Laboratory of Spinal Disease Research, Peking University Third Hospital, Beijing, China.
Orthop Surg. 2024 Apr;16(4):830-841. doi: 10.1111/os.13973. Epub 2024 Feb 21.
Degenerative thoracolumbar hyperkyphosis (DTH) is a disease that negatively affects individual health and requires surgical intervention, yet the ideal surgical approach and complications, especially distal junctional failures (DJF), remain poorly understood. This study aims to investigate DJF in DTH and to identify the risk factors for DJF so that we can improve surgical decision-making, and advance our knowledge in the field of spinal surgery to enhance patient outcomes.
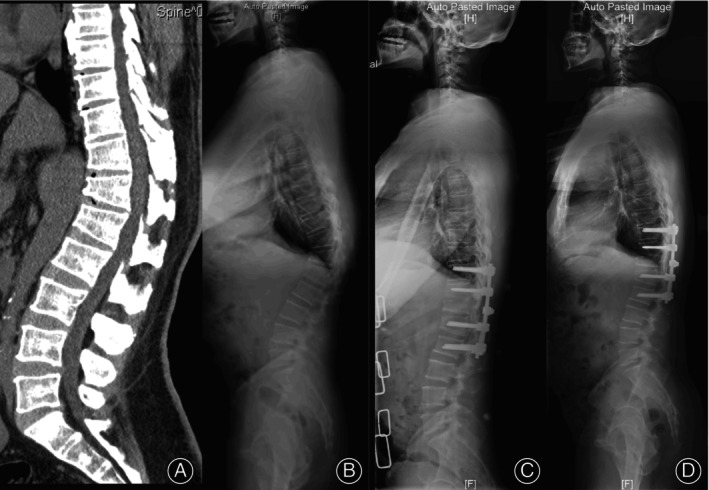
This study retrospectively reviewed 78 cases (late osteoporotic vertebral compression fracture [OVCF], 51; Scheuermann's kyphosis [SK], 17; and degenerative disc diseases [DDD], 10) who underwent corrective surgery in our institute from 2008 to 2019. Clinical outcomes were assessed using health-related quality of life (HRQOL) measures, including the visual analogue scale (VAS) scores for back and leg pain, the Oswestry disability index (ODI), and the Japanese Orthopaedic Association (JOA) scoring system. Multiple radiographic parameters, such as global kyphosis (GK) and thoracolumbar kyphosis (TLK), were assessed to determine radiographic outcomes. Multivariate logistic regression analysis was employed to identify the risk factors associated with DJF.
HRQOL improved, and GK, TLK decreased at the final follow-up, with a correction rate of 67.7% and 68.5%, respectively. DJF was found in 13 of 78 cases (16.7%), two cases had wedging in the disc (L3-4) below the instrumentation, one case had a fracture of the lowest instrumented vertebrae (LIV), one case had osteoporotic fracture below the fixation, nine cases had pull-out or loosening of the screws at the LIV and three cases (23.1%) required revision surgery. The DJF group had older age, lower computed tomography Hounsfield unit (CT HU), longer follow-up, more blood loss, greater preoperative sagittal vertical axis (SVA), and poorer postoperative JOA and VAS scores (back). The change in TLK level was larger in the non-DJF group. Post-sagittal stable vertebrae (SSV) moved cranially compared with pre-SSV.
Age, CT HU, length of follow-up, estimated blood loss, and preoperative SVA were independent risk factors for DJF. We recommend fixation of the two vertebrae below the apex vertebrae for DTH to minimize surgical trauma.
退变性胸腰椎后凸(DTH)是一种对个体健康有负面影响且需要手术干预的疾病,但理想的手术方法和并发症,特别是远端交界性失败(DJF),仍知之甚少。本研究旨在探讨 DTH 中的 DJF,并确定 DJF 的危险因素,以便我们能够改进手术决策,并在脊柱外科领域推进知识,以改善患者的预后。
本研究回顾性分析了 2008 年至 2019 年在我院接受矫正手术的 78 例病例(晚期骨质疏松性椎体压缩性骨折[OVCF]51 例,Scheuermann 后凸[SK]17 例,退行性椎间盘疾病[DDD]10 例)。使用健康相关生活质量(HRQOL)量表评估临床结果,包括背部和腿部疼痛的视觉模拟评分(VAS)、Oswestry 残疾指数(ODI)和日本矫形协会(JOA)评分系统。评估了多个放射学参数,如总体后凸(GK)和胸腰椎后凸(TLK),以确定放射学结果。采用多变量逻辑回归分析确定与 DJF 相关的危险因素。
在最终随访时,HRQOL 得到改善,GK 和 TLK 降低,校正率分别为 67.7%和 68.5%。在 78 例中发现 DJF 13 例(16.7%),2 例(L3-4 椎间盘)下方器械处发生楔形变,1 例最下方置钉椎体骨折,1 例固定下方骨质疏松性骨折,9 例 LIV 处螺钉拔出或松动,3 例(23.1%)需要翻修手术。DJF 组年龄较大,CT 亨氏单位(CT HU)较低,随访时间较长,失血量较大,术前矢状垂直轴(SVA)较大,术后 JOA 和 VAS 评分(背部)较差。非 DJF 组 TLK 水平变化较大。与术前 SSV 相比,后矢状稳定椎体(SSV)向头侧移动。
年龄、CT HU、随访时间、估计失血量和术前 SVA 是 DJF 的独立危险因素。我们建议对 DTH 进行上下两个椎体的固定,以最大限度地减少手术创伤。