K. Y. H. Kwan, The University of Hong Kong, Pokfulam, Hong Kong.
L. G. Lenke, Columbia University Medical Center, New York, NY, USA.
Clin Orthop Relat Res. 2021 Feb 1;479(2):312-320. doi: 10.1097/CORR.0000000000001521.
The Global Alignment and Proportion (GAP) score, based on pelvic incidence-based proportional parameters, was recently developed to predict mechanical complications after surgery for spinal deformities in adults. However, this score has not been validated in an independent external dataset.
QUESTIONS/PURPOSES: After adult spinal deformity surgery, is a higher GAP score associated with (1) an increased risk of mechanical complications, defined as rod fractures, implant-related complications, proximal or distal junctional kyphosis or failure; (2) a higher likelihood of undergoing revision surgery to treat a mechanical complication; and (3) is a lower (more proportioned) GAP score category associated with better validated outcomes scores using the Oswestry Disability Index (ODI), Scoliosis Research Society-22 (SRS-22) and the Short Form-36 questionnaires?
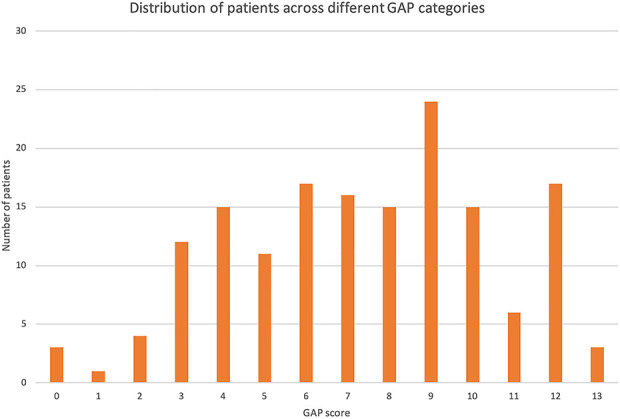
A total of 272 patients who had undergone corrective surgeries for complex spinal deformities were enrolled in the Scoli-RISK-1 prospective trial. Patients were included in this secondary analysis if they fulfilled the original inclusion criteria by Yilgor et al. From the original 272 patients, 14% (39) did not satisfy the radiographic inclusion criteria, the GAP score could not be calculated in 14% (37), and 24% (64) did not have radiographic assessment at postoperative 2 years, leaving 59% (159) for analysis in this review of data from the original trial. A total of 159 patients were included in this study,with a mean age of 58 ± 14 years at the time of surgery. Most patients were female (72%, 115 of 159), the mean number of levels involved in surgery was 12 ± 4, and three-column osteotomy was performed in 76% (120 of 159) of patients. The GAP score was calculated using parameters from early postoperative radiographs (between 3 and 12 weeks) including pelvic incidence, sacral slope, lumbar lordosis, lower arc lordosis and global tilt, which were independently obtained from a computer software based on centralized patient radiographs. The GAP score was categorized as proportional (scores of 0 to 2), moderately disproportional (scores of 3 to 6), or severely disproportional (scores higher than 7 to 13). Receiver operating characteristic area under curve (AUC) was used to assess associations between GAP score and risk of mechanical complications and risk of revision surgery. An AUC of 0.5 to 0.7 was classified as "no or low associative power", 0.7 to 0.9 as "moderate" and greater than 0.9 as "high". We analyzed differences in validated outcome scores between the GAP categories using Wilcoxon rank sum test.
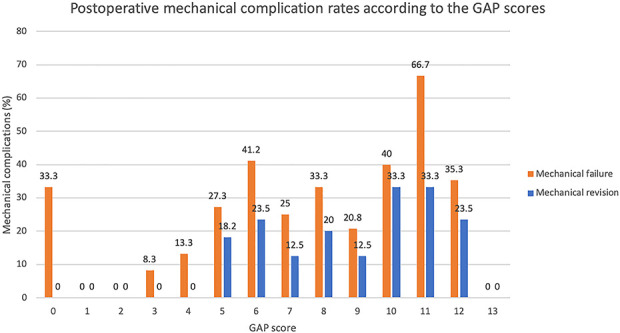
At a minimum of 2 years' follow-up, a higher GAP score was not associated with increased risks of mechanical complications (AUC = 0.60 [95% CI 0.50 to 0.70]). A higher GAP score was not associated with a higher likelihood of undergoing a revision surgery to treat a mechanical complication (AUC = 0.66 [95% 0.53 to 0.78]). However, a moderately disproportioned GAP score category was associated with better SF-36 physical component summary score (36 ± 10 versus 40 ± 11; p = 0.047), better SF-36 mental component summary score (46 ± 13 versus 51 ± 12; p = 0.01), better SRS-22 total score (3.4 ± 0.8 versus 3.7 ± 0.7, p = 0.02) and better ODI score (35 ± 21 versus 25 ± 20; p = 0.003) than severely disproportioned GAP score category.
Based on the findings of this external validation study, we found that alignment targets based on the GAP score alone were not associated with increased risks of mechanical complications and mechanical revisions in patients with complex adult spinal disorders. Parameters not included in the original GAP score needed to be considered to reduce the likelihood of mechanical complications.
Level III, diagnostic study.
基于基于骨盆入射角的比例参数的全局对准和比例(GAP)评分,最近被开发出来用于预测成人脊柱畸形手术后的机械并发症。然而,该评分尚未在独立的外部数据集进行验证。
问题/目的:成人脊柱畸形手术后,(1)更高的 GAP 评分是否与机械并发症的风险增加相关,机械并发症定义为杆断裂、植入物相关并发症、近端或远端交界性后凸或失败;(2)更高的可能性需要进行翻修手术来治疗机械并发症;以及(3)较低(更成比例)的 GAP 评分类别是否与使用 Oswestry 残疾指数(ODI)、脊柱侧凸研究协会-22(SRS-22)和简短形式-36 问卷的更好验证结果评分相关?
共有 272 名接受复杂脊柱畸形矫正手术的患者被纳入 Scoli-RISK-1 前瞻性试验。如果 Yilgor 等人的原始纳入标准满足,患者将被纳入这项二次分析。在最初的 272 名患者中,14%(39 名)不符合放射学纳入标准,14%(37 名)无法计算 GAP 评分,24%(64 名)在术后 2 年时没有进行放射学评估,因此在对原始试验数据的回顾中,59%(159 名)可用于分析。共有 159 名患者纳入本研究,平均年龄为手术时 58±14 岁。大多数患者为女性(72%,115/159),手术涉及的平均节段数为 12±4,76%(120/159)的患者行三柱截骨术。GAP 评分使用术后早期(3 至 12 周)的放射学参数计算,包括骨盆入射角、骶骨倾斜度、腰椎前凸度、下弧前凸度和整体倾斜度,这些参数均由基于患者放射学的计算机软件独立获得。GAP 评分分为比例(评分 0 至 2)、中度不成比例(评分 3 至 6)或严重不成比例(评分高于 7 至 13)。接受者操作特征曲线(AUC)用于评估 GAP 评分与机械并发症风险和机械翻修手术风险之间的关系。AUC 为 0.5 至 0.7 被归类为“无或低关联能力”,0.7 至 0.9 为“中等”,大于 0.9 为“高”。我们使用 Wilcoxon 秩和检验分析 GAP 分类之间验证后结果评分的差异。
在至少 2 年的随访中,较高的 GAP 评分与机械并发症风险增加无关(AUC = 0.60 [95%CI 0.50 至 0.70])。较高的 GAP 评分与机械并发症需要进行翻修手术的可能性增加无关(AUC = 0.66 [95%CI 0.53 至 0.78])。然而,中度不成比例的 GAP 评分类别与更好的 SF-36 物理成分综合评分(36±10 与 40±11;p = 0.047)、更好的 SF-36 心理成分综合评分(46±13 与 51±12;p = 0.01)、更好的 SRS-22 总评分(3.4±0.8 与 3.7±0.7,p = 0.02)和更好的 ODI 评分(35±21 与 25±20;p = 0.003)相关,而严重不成比例的 GAP 评分类别与更好的 SF-36 物理成分综合评分(36±10 与 40±11;p = 0.047)、更好的 SF-36 心理成分综合评分(46±13 与 51±12;p = 0.01)、更好的 SRS-22 总评分(3.4±0.8 与 3.7±0.7,p = 0.02)和更好的 ODI 评分(35±21 与 25±20;p = 0.003)相关。
基于这项外部验证研究的结果,我们发现基于 GAP 评分的对准目标与复杂成人脊柱疾病患者的机械并发症和机械翻修风险增加无关。需要考虑原始 GAP 评分中未包含的参数,以降低机械并发症的可能性。
III 级,诊断研究。