El-Hajj Victor Gabriel, Ghaith Abdul Karim, Nguyen Ryan H, Al-Saidi Neil Nazar, Hoang Harry, Graepel Stephen P, Elmi-Terander Adrian, Lehrer Eric J, Brown Paul, Bydon Mohamad
Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden.
Mayo Clinic Neuro-Informatics Laboratory, Mayo Clinic, Rochester, Minnesota, USA.
Neurooncol Adv. 2024 Feb 5;6(1):vdae018. doi: 10.1093/noajnl/vdae018. eCollection 2024 Jan-Dec.
Although typically benign, 5% of spinal meningiomas (SMs) present with higher-grade features (World Health Organization grades 2 and 3). High-grade SMs are poorly studied and the role of adjuvant radiotherapy in their management remains controversial. We hence aimed to study the demographic characteristics of this rare tumor and investigate the outcomes associated with the use of surgery with adjuvant therapy in contrast to surgery alone.
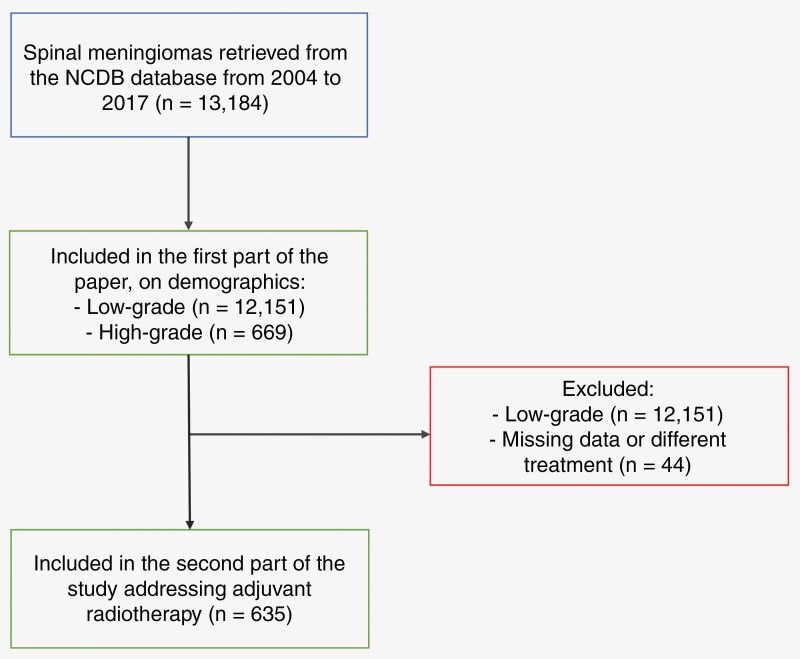
The National Cancer Database was queried for patients with SMs from 2004 to 2017. Basic statistics were used to identify differences between low- and high-grade tumors in terms of baseline characteristics. Surgery with and without adjuvant radiotherapy were compared after (1:1) propensity-score matching. Kaplan-Meier survival analysis was conducted to study overall survival. All analyses were performed on R.
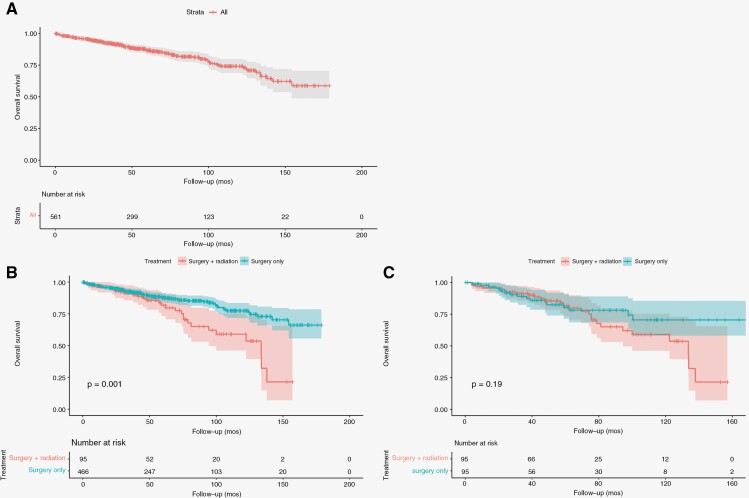
A total of 13 184 patients diagnosed with SMs were included, of whom only 5% ( = 669) had high-grade SMs. Patients with high-grade SMs presented at a younger median age (57 years [IQR: 44-68] versus 65 years [54-75]; < .001) and were more commonly males (33% vs 20%; < .001). After propensity-score matching, survival analysis revealed similar overall survival outcomes in patients with high-grade SM undergoing both surgery and radiotherapy as compared to those only receiving surgery ( = .19).
This study reveals major demographic differences between high- and low-grade SMs. There were no benefits associated with the use of adjuvant radiotherapy. However, due to confounding, overall survival outcomes between patients receiving surgery alone and those receiving surgery with adjuvant radiotherapy are not causally interpretable.
虽然脊髓膜瘤(SMs)通常为良性,但5%的脊髓膜瘤具有高级别特征(世界卫生组织2级和3级)。高级别脊髓膜瘤的研究较少,辅助放疗在其治疗中的作用仍存在争议。因此,我们旨在研究这种罕见肿瘤的人口统计学特征,并调查与单纯手术相比,手术联合辅助治疗的效果。
查询2004年至2017年国家癌症数据库中脊髓膜瘤患者的信息。使用基本统计方法确定低级别和高级别肿瘤在基线特征方面的差异。在进行(1:1)倾向评分匹配后,比较接受和未接受辅助放疗的手术情况。采用Kaplan-Meier生存分析来研究总生存期。所有分析均在R软件上进行。
共纳入13184例诊断为脊髓膜瘤的患者,其中只有5%(n = 669)为高级别脊髓膜瘤。高级别脊髓膜瘤患者的中位年龄较小(57岁[四分位间距:44 - 68]对65岁[54 - 75];P <.001),男性更为常见(33%对20%;P <.001)。倾向评分匹配后,生存分析显示,接受手术和放疗的高级别脊髓膜瘤患者与仅接受手术的患者相比,总生存结果相似(P = 0.19)。
本研究揭示了高级别和低级别脊髓膜瘤在主要人口统计学方面的差异。使用辅助放疗没有益处。然而,由于存在混杂因素,单纯接受手术的患者与接受手术联合辅助放疗的患者之间的总生存结果无法进行因果解释。