Department of Gastroenterology, Hiroshima University Hospital, 1-2-3, Kasumi, Minami-Ku, Hiroshima, 734-8551, Japan.
Department of Gastrointestinal and Hepato-Biliary-Pancreatic Surgery, Nippon Medical School, Tokyo, Japan.
J Gastroenterol. 2024 May;59(5):376-388. doi: 10.1007/s00535-024-02081-3. Epub 2024 Feb 27.
The clinicopathological features and prognosis of primary small bowel adenocarcinoma (PSBA), excluding duodenal cancer, remain undetermined due to its rarity in Japan.
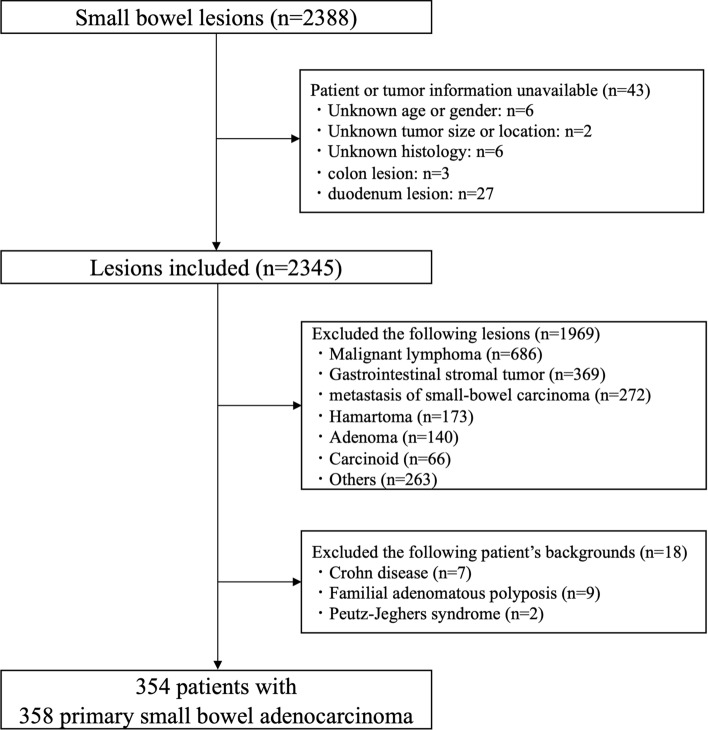
We analyzed 354 patients with 358 PSBAs, between January 2008 and December 2017, at 44 institutions affiliated with the Japanese Society for Cancer of the Colon and Rectum.
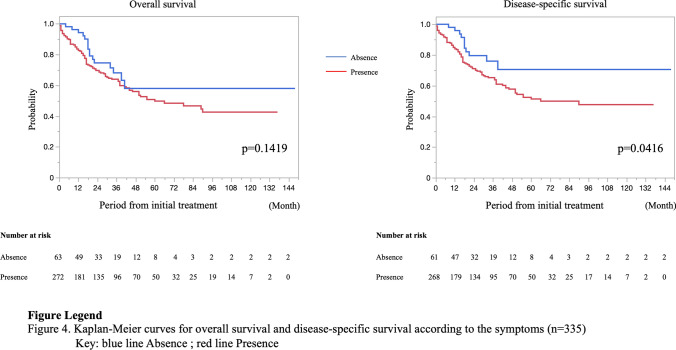
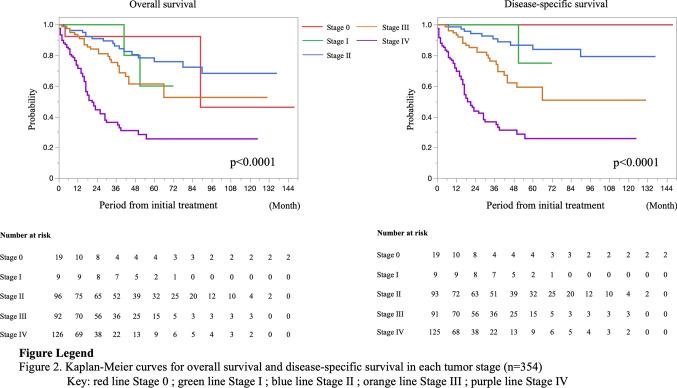
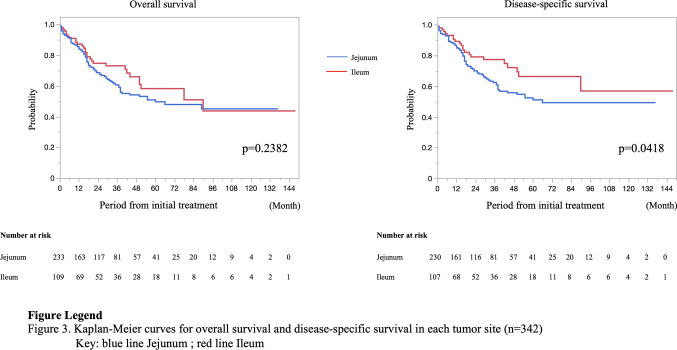
The median age was 67 years (218 males, 61.6%). The average tumor size was 49.9 (7-100) mm. PSBA sites consisted of jejunum (66.2%) and ileum (30.4%). A total of 219 patients (61.9%) underwent diagnostic small bowel endoscopy, including single-balloon endoscopy, double-balloon endoscopy, and capsule endoscopy before treatment. Nineteen patients (5.4%) had Lynch syndrome, and 272 patients (76.8%) had symptoms at the initial diagnosis. The rates for stages 0, I, II, III, and IV were 5.4%, 2.5%, 27.1%, 26.0%, and 35.6%, respectively. The 5-year overall survival rates at each stage were 92.3%, 60.0%, 75.9%, 61.4%, and 25.5%, respectively, and the 5-year disease-specific survival (DSS) rates were 100%, 75.0%, 84.1%, 59.3%, and 25.6%, respectively. Patients with the PSBA located in the jejunum, with symptoms at the initial diagnosis or advanced clinical stage had a worse prognosis. However, multivariate analysis using Cox-hazard model revealed that clinical stage was the only significant predictor of DSS for patients with PSBA.
Of the patients with PSBA, 76.8% had symptoms at the initial diagnosis, which were often detected at an advanced stage. Detection during the early stages of PSBA is important to ensure a good prognosis.
原发性小肠腺癌(PSBA)除十二指肠癌外,在日本较为罕见,其临床病理特征和预后仍不明确。
我们分析了 2008 年 1 月至 2017 年 12 月期间,日本癌症协会结肠癌和直肠癌分会 44 家机构的 354 例 PSBA 患者(358 例)。
中位年龄为 67 岁(218 例男性,61.6%)。肿瘤平均直径为 49.9(7-100)mm。PSBA 部位包括空肠(66.2%)和回肠(30.4%)。219 例患者(61.9%)在治疗前接受了诊断性小肠内镜检查,包括单气囊内镜、双气囊内镜和胶囊内镜。19 例患者(5.4%)存在林奇综合征,272 例患者(76.8%)在初始诊断时出现症状。0 期、Ⅰ期、Ⅱ期、Ⅲ期和Ⅳ期的比例分别为 5.4%、2.5%、27.1%、26.0%和 35.6%。各期的 5 年总生存率分别为 92.3%、60.0%、75.9%、61.4%和 25.5%,5 年疾病特异性生存率(DSS)分别为 100%、75.0%、84.1%、59.3%和 25.6%。空肠部位、初始诊断时出现症状或临床分期较晚的 PSBA 患者预后较差。然而,采用 Cox 风险模型的多变量分析显示,临床分期是 PSBA 患者 DSS 的唯一显著预测因素。
PSBA 患者中 76.8%在初始诊断时出现症状,这些症状往往在晚期出现。在 PSBA 的早期阶段进行检测对确保良好的预后非常重要。