Mendes Pedro Diogo, Paulo Sérgio Eduardo, Santos Carla Mimoso, Fonseca Ana Bruschy, Melo Cristino José, Pereira Álvaro Ayres, Caneiras Cátia
Serviço de Doenças Infeciosas, Centro Hospitalar Universitário Lisboa Norte EPE, Lisbon, Portugal.
Clínica Universitária de Doenças Infeciosas, Faculdade de Medicina da Universidade de Lisboa, Lisbon, Portugal.
Front Microbiol. 2024 Feb 13;15:1347521. doi: 10.3389/fmicb.2024.1347521. eCollection 2024.
Extensively drug-resistant (XDR-PA) is a growing concern due to its increasing incidence, limited therapeutic options, limited data on the optimal treatment, and high mortality rates. The study aimed to characterize the population, the outcome and the microbiological characteristics of XDR-PA identified in a Portuguese university hospital center.
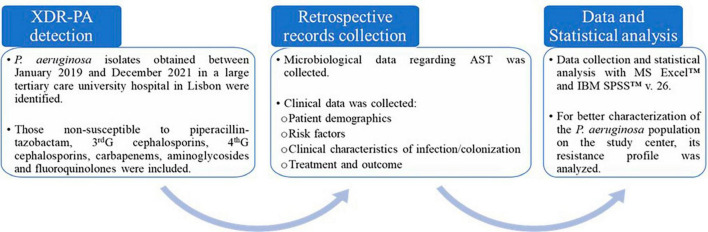
All XDR-PA isolates between January 2019 and December 2021 were identified. XDR-PA was defined as resistance to piperacillin-tazobactam, third and fourth generation cephalosporins, carbapenems, aminoglycosides and fluoroquinolones. A retrospective analysis of the medical records was performed.
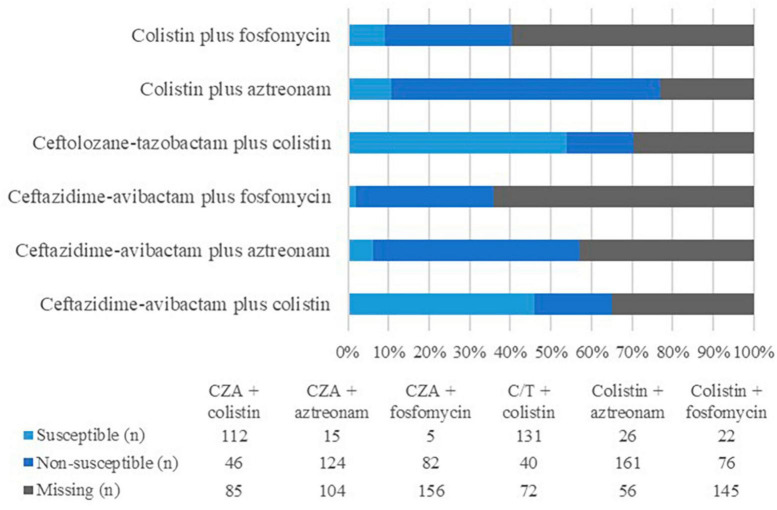
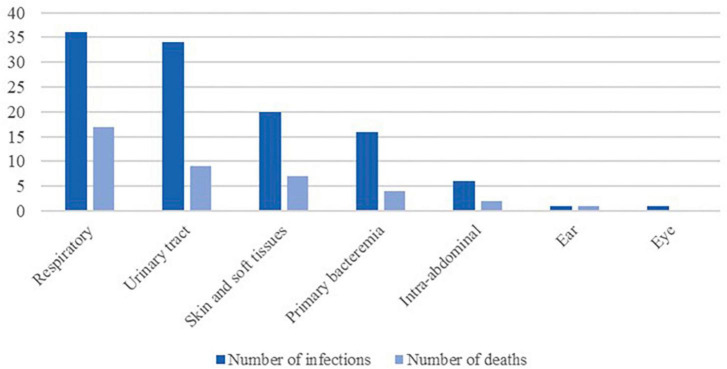
One hundred seventy-eight individual episodes among 130 patients with XDR-PA detection were identified. The most common sources of infection were respiratory (32%) and urinary tracts (30%), although skin and soft tissue infections (18%) and primary bacteremia (14%) were also prevalent. Colonization was admitted in 64 cases. Several patients had risk factors for complicated infections, most notably immunosuppression, structural lung abnormalities, major surgery, hemodialysis or foreign intravascular or urinary devices. XDR-PA identification was more frequent in male patients with an average age of 64.3 ± 17.5 years. One non-susceptibility to colistin was reported. Only 12.4% were susceptible to aztreonam. Ceftazidime-avibactam (CZA) was susceptible in 71.5% of the tested isolates. Ceftolozane-tazobactam (C/T) was susceptible in 77.5% of the tested isolates. Antibiotic regimens with XDR-PA coverage were reserved for patients with declared infection, except to cystic fibrosis. The most frequently administered antibiotics were colistin (41 cases), CZA (39 cases), and C/T (16 cases). When combination therapy was used, CZA plus colistin was preferred. The global mortality rate among infected patients was 35.1%, significantly higher in those with hematologic malignancy (50.0%, < 0.05), followed by the ones with bacteremia (44.4%, < 0.05) and those medicated with colistin (39.0%, < 0.05), especially the ones with respiratory infections (60.0%). Among patients treated with CZA or C/T, the mortality rate seemed to be lower.
XDR-PA infections can be severe and difficult to treat, with a high mortality rate. Even though colistin seems to be a viable option, it is likely less safe and efficient than CZA and C/T. To the best of the authors' knowledge, this is the first description of the clinical infection characteristics and treatment of XDR-PA in Portugal.
广泛耐药性鲍曼不动杆菌(XDR-PA)因其发病率不断上升、治疗选择有限、关于最佳治疗的数据有限以及高死亡率而日益受到关注。本研究旨在描述在一家葡萄牙大学医院中心鉴定出的XDR-PA的人群、结局和微生物学特征。
鉴定了2019年1月至2021年12月期间所有的XDR-PA分离株。XDR-PA被定义为对哌拉西林-他唑巴坦、第三代和第四代头孢菌素、碳青霉烯类、氨基糖苷类和氟喹诺酮类耐药。对病历进行了回顾性分析。
在130例检测出XDR-PA的患者中,共鉴定出178例个体感染事件。最常见的感染源是呼吸道(32%)和泌尿道(30%),尽管皮肤和软组织感染(18%)和原发性菌血症(14%)也很常见。64例患者存在定植情况。一些患者有复杂感染的危险因素,最显著的是免疫抑制、结构性肺部异常、大手术、血液透析或血管内或泌尿道异物。XDR-PA在平均年龄为64.3±17.5岁的男性患者中更常见。报告了1例对黏菌素不敏感的情况。仅12.4%对氨曲南敏感。头孢他啶-阿维巴坦(CZA)在71.5%的检测分离株中敏感。头孢洛扎坦-他唑巴坦(C/T)在77.5%的检测分离株中敏感。除囊性纤维化患者外,针对XDR-PA感染的抗生素治疗方案仅用于确诊感染的患者。最常用的抗生素是黏菌素(41例)、CZA(39例)和C/T(16例)。当采用联合治疗时,首选CZA加黏菌素。感染患者的总体死亡率为35.1%,血液系统恶性肿瘤患者的死亡率显著更高(50.0%,P<0.05),其次是菌血症患者(44.4%,P<0.05)和使用黏菌素治疗的患者(39.0%,P<0.05),尤其是呼吸道感染患者(60.0%)。在接受CZA或C/T治疗的患者中,死亡率似乎较低。
XDR-PA感染可能很严重且难以治疗,死亡率很高。尽管黏菌素似乎是一种可行的选择,但它可能不如CZA和C/T安全有效。据作者所知,这是葡萄牙首次对XDR-PA的临床感染特征和治疗进行的描述。