Department of Nephrology, Odense University Hospital, Odense, Denmark.
Department of Nephrology, Aarhus University Hospital, Aarhus, Denmark.
Clin J Am Soc Nephrol. 2024 Jun 1;19(6):755-766. doi: 10.2215/CJN.0000000000000439. Epub 2024 Feb 27.
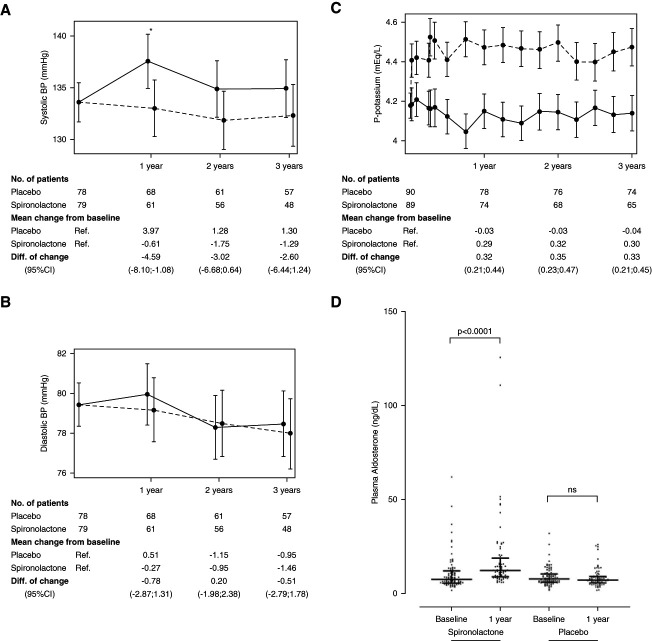
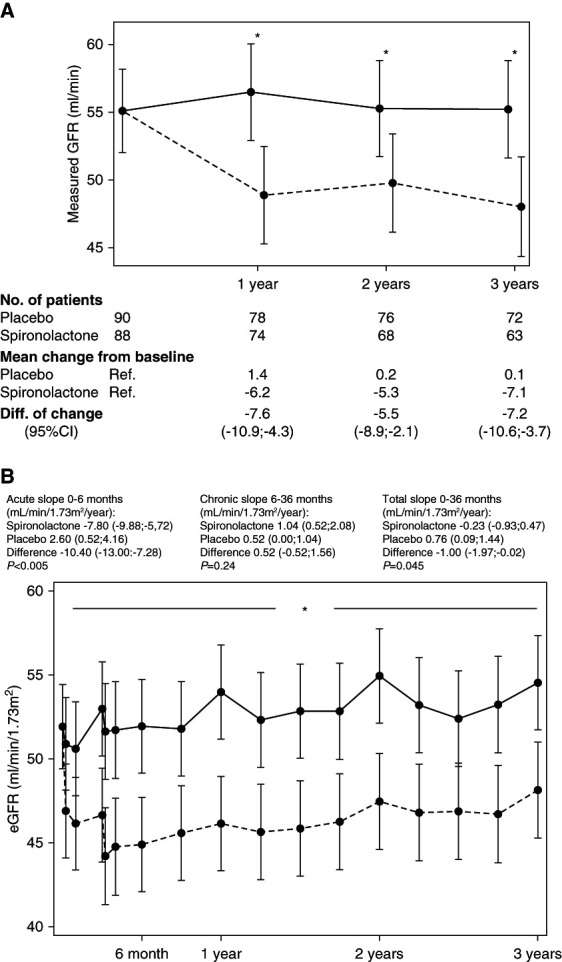
Spironolactone is safe for kidney transplant patients. Spironolactone reduces kidney function by an acute effect, whereafter it remains stable. Spironolactone does not affect the progression of interstitial fibrosis in protocol biopsies.
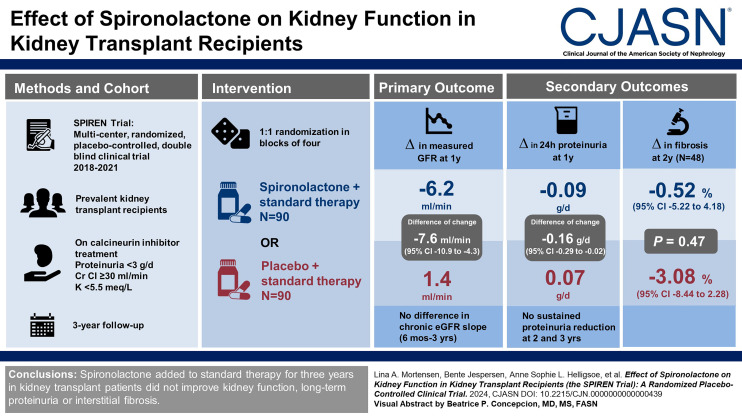
Long-term kidney allograft survival is hampered by progressive interstitial fibrosis and tubular atrophy. The SPIREN trial tested the hypothesis that the mineralocorticoid receptor antagonist spironolactone stabilizes kidney function and attenuates glomerular barrier injury in kidney transplant patients treated with calcineurin inhibitors.
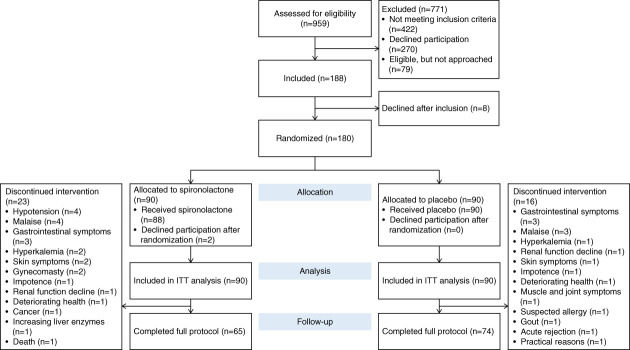
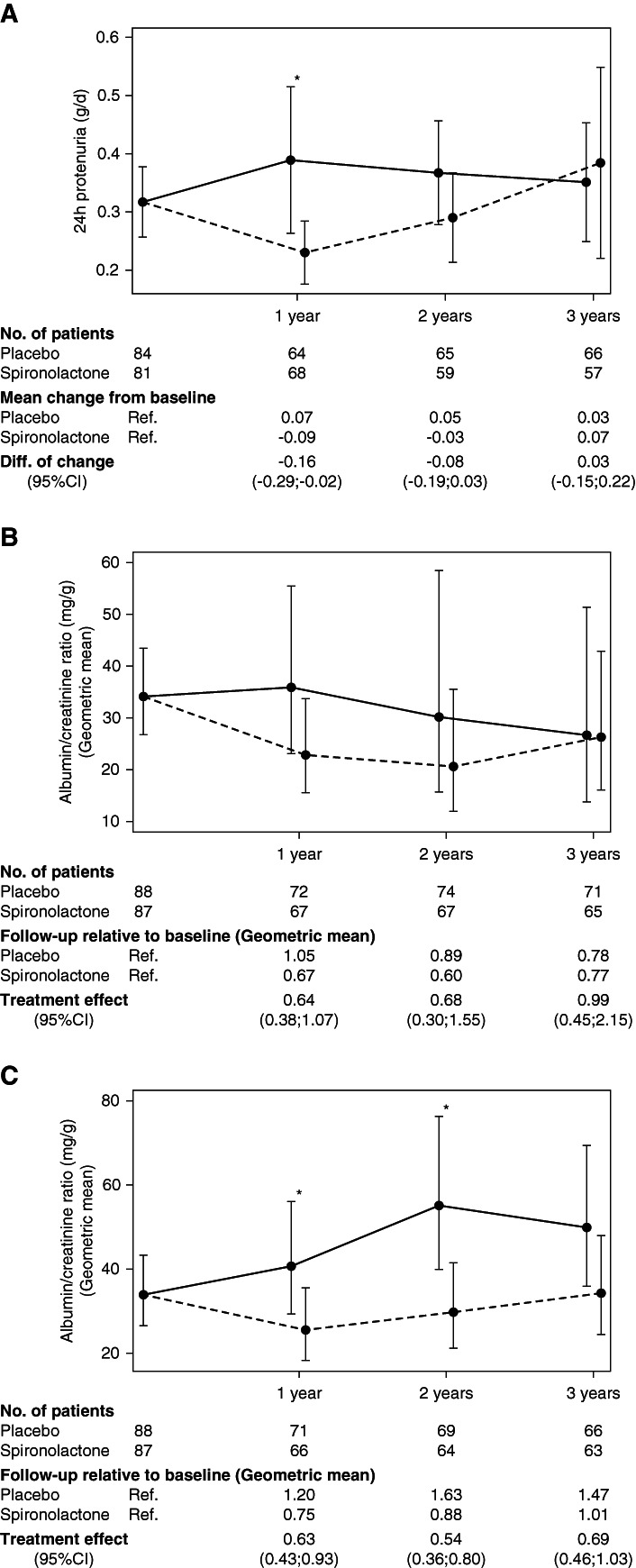
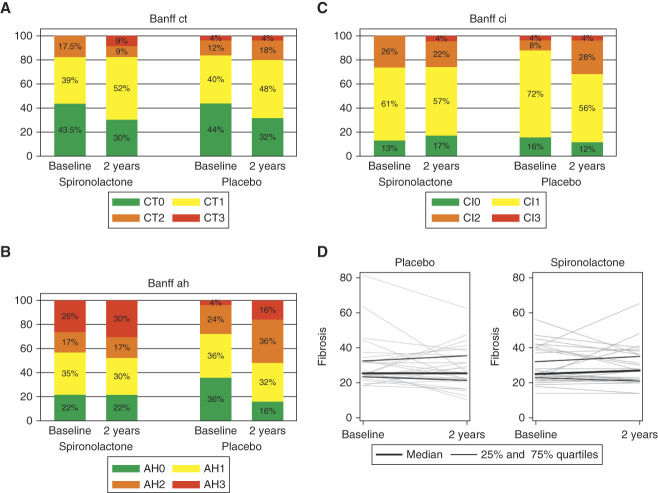
We conducted a randomized, placebo-controlled, double-blind clinical trial including 188 prevalent kidney transplant patients. Patients were randomized to spironolactone or placebo for 3 years. GFR was measured along with proteinuria and kidney fibrosis. The primary end point was change in measured GFR. Secondary outcomes were 24-hour proteinuria, kidney allograft fibrosis, and cardiovascular events. Measured GFRs, 24-hour proteinuria, and BP were determined yearly. Kidney biopsies were collected at baseline and after 2 years (=48). Fibrosis was evaluated by quantitative stereology and classified according to Banff.
The groups were comparable at baseline except for slightly older allografts in the spironolactone group. Spironolactone reduced measured GFRs (up to –7.6 [95% confidence interval, −10.9 to −4.3] ml/min compared with placebo) independently of time since transplantation and BP with no effect on the kidney function curve over time and reduced 24-hour proteinuria after 1 year. There was no significant effect of spironolactone on the development of interstitial fibrosis.
Spironolactone added to standard therapy for 3 years in kidney transplant patients did not improve kidney function, long-term proteinuria, or interstitial fibrosis.
NCT01602861.
螺内酯可用于肾移植患者且安全。螺内酯通过急性效应降低肾功能,随后保持稳定。螺内酯不会影响方案活检中间质纤维化的进展。
长期的肾移植存活率受到进行性间质纤维化和肾小管萎缩的阻碍。SPIREN 试验检验了假设,即醛固酮受体拮抗剂螺内酯稳定肾功能并减轻接受钙调磷酸酶抑制剂治疗的肾移植患者的肾小球屏障损伤。
我们进行了一项随机、安慰剂对照、双盲临床试验,纳入了 188 例现患肾移植患者。患者随机接受螺内酯或安慰剂治疗 3 年。肾小球滤过率(GFR)与蛋白尿和肾纤维化一起测量。主要终点是测量 GFR 的变化。次要终点是 24 小时蛋白尿、肾移植纤维化和心血管事件。每年测量 GFR、24 小时蛋白尿和血压。基线和 2 年后(=48 个月)采集肾活检。通过定量体视学评估纤维化,并根据 Banff 进行分类。
除了螺内酯组的移植物稍老化外,两组在基线时具有可比性。螺内酯降低了测量的 GFR(与安慰剂相比,降低了-7.6[95%置信区间,-10.9 至-4.3]ml/min),与移植时间和血压无关,对随时间推移的肾功能曲线没有影响,并在 1 年后降低了 24 小时蛋白尿。螺内酯对间质纤维化的发展没有显著影响。
在肾移植患者的标准治疗中添加螺内酯 3 年并未改善肾功能、长期蛋白尿或间质纤维化。
NCT01602861。