Fagereng Gro Live, Morvik Anne Marit, Reinvik Ulimoen Sara, Ringerud Anne Marthe, Dahlen Syversen Iselin, Sagdahl Erik
The Pharmaceutical Division, The Norwegian Hospital Procurement Trust, Vadsø, Norway.
Institute for Cancer Research, Division of Cancer Medicine, Oslo University Hospital, Oslo, Norway.
Front Pharmacol. 2024 Feb 14;15:1338541. doi: 10.3389/fphar.2024.1338541. eCollection 2024.
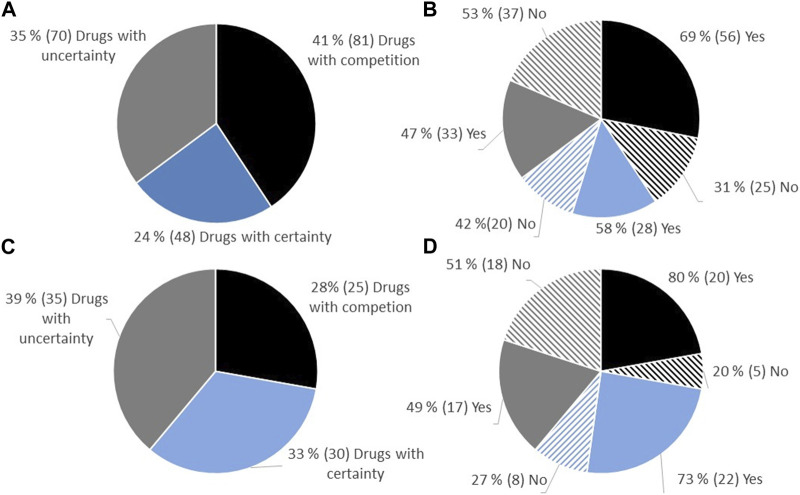
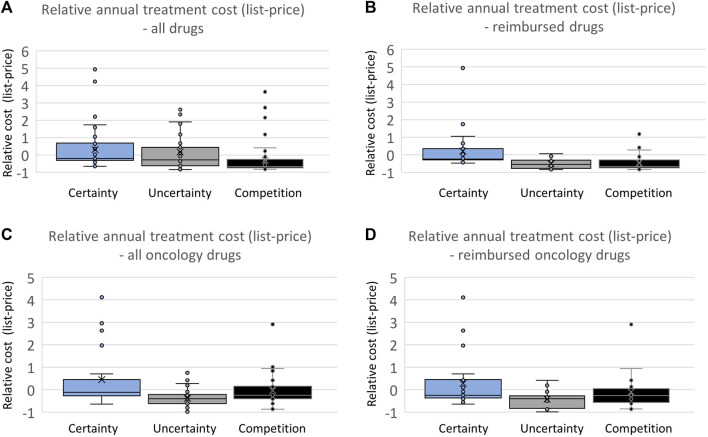
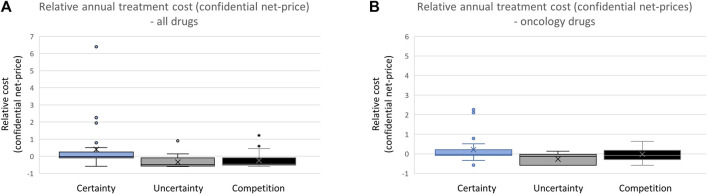
Over the preceding decade, an increasing number of drugs have been approved by the European Medicines Agency (EMA) with limited knowledge of their relative efficacy. This is due to the utilization of non-randomized, single-arm studies, surrogate endpoints, and shorter follow-up time. The impact of this trend on the accessibility and affordability of newly approved drugs in Europe remains uncertain. The primary objective of this study is to provide insights into the issues of accessibility and affordability of new drugs in the Norwegian healthcare system. The presented study entails an analysis of all reimbursement decisions for hospital drugs in Norway spanning 2021-2022. The included drugs were approved by the EMA between 2014 and 2022, with the majority (91%) receiving approval between 2018 and 2022. The drugs were categorized based on the level of documentation of relative efficacy. Approval rates and costs (confidential net-prices) were compared. A total of 35% (70/199) of the reimbursement decisions were characterized by limited certainty regarding relative efficacy and as a consequence the Norwegian Health Technology Assessment (HTA) body did not present an incremental cost-effectiveness ratio (ICER) in the HTA report. Within this category, a lower percentage of drugs (47%) gained reimbursement approval compared to those with a higher certainty level, which were presented with an ICER (58%). On average, drugs with an established relative efficacy were accepted with a 4.4-fold higher cost (confidential net-prices). These trends persisted when specifically examining oncology drugs. Our study underscores that a substantial number of recently introduced drugs receive reimbursement regardless of the level of certainty concerning relative efficacy. However, the results suggest that payers prioritize documented over potential efficacy. Given that updated information on relative efficacy may emerge post-market access, a potential solution to address challenges related to accessibility and affordability in Europe could involve an increased adoption of market entry agreements. These agreements could allow for price adjustments after the presentation of new knowledge regarding relative efficacy, potentially resolving some of the current challenges.
在过去十年中,越来越多的药物在对其相对疗效了解有限的情况下获得了欧洲药品管理局(EMA)的批准。这是由于采用了非随机单臂研究、替代终点以及较短的随访时间。这种趋势对欧洲新批准药物的可及性和可负担性的影响仍不确定。本研究的主要目的是深入了解挪威医疗保健系统中新药的可及性和可负担性问题。本研究对2021年至2022年挪威所有医院药物报销决定进行了分析。纳入的药物在2014年至2022年期间获得了EMA的批准,其中大多数(91%)在2018年至2022年期间获得批准。这些药物根据相对疗效的文献记录水平进行分类。比较了批准率和成本(保密净价)。共有35%(70/199)的报销决定的特点是相对疗效的确定性有限,因此挪威卫生技术评估(HTA)机构在HTA报告中未给出增量成本效益比(ICER)。在这一类别中,与具有较高确定性水平且给出ICER的药物(58%)相比,获得报销批准的药物比例较低(47%)。平均而言,具有已确定相对疗效的药物被接受的成本(保密净价)高出4.4倍。在专门研究肿瘤药物时,这些趋势依然存在。我们的研究强调,大量最近引入的药物无论相对疗效的确定性水平如何都能获得报销。然而,结果表明,支付方优先考虑有记录的疗效而非潜在疗效。鉴于上市后可能会出现关于相对疗效的最新信息,解决欧洲可及性和可负担性相关挑战的一个潜在解决方案可能是更多地采用市场准入协议。这些协议可以在出现关于相对疗效的新知识后进行价格调整,有可能解决一些当前的挑战。