Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India
Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Eur Respir J. 2024 Apr 4;63(4). doi: 10.1183/13993003.00061-2024. Print 2024 Apr.
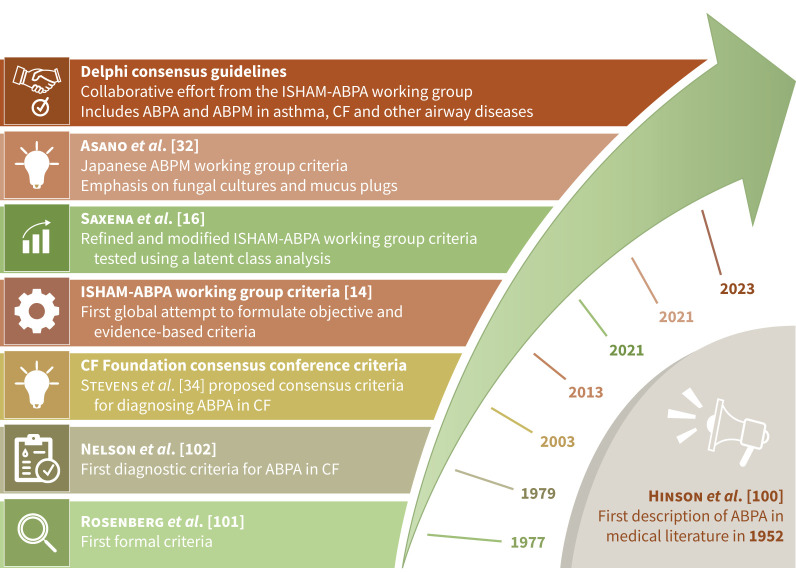
The International Society for Human and Animal Mycology (ISHAM) working group proposed recommendations for managing allergic bronchopulmonary aspergillosis (ABPA) a decade ago. There is a need to update these recommendations due to advances in diagnostics and therapeutics.
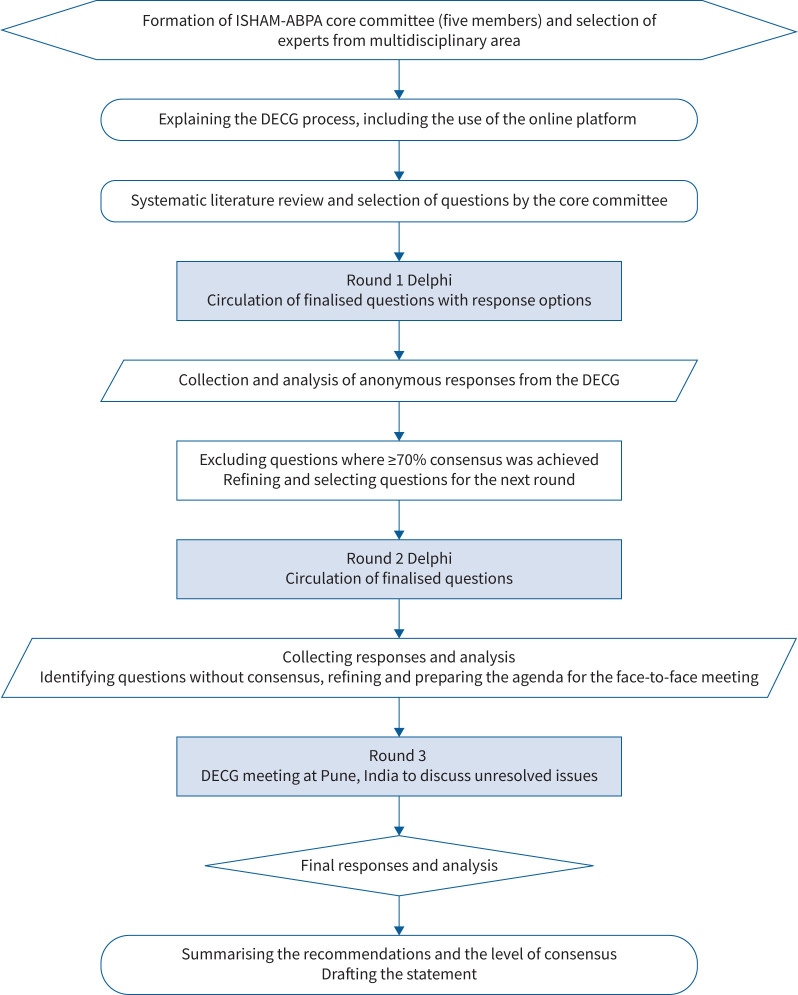
An international expert group was convened to develop guidelines for managing ABPA (caused by spp.) and allergic bronchopulmonary mycosis (ABPM; caused by fungi other than spp.) in adults and children using a modified Delphi method (two online rounds and one in-person meeting). We defined consensus as ≥70% agreement or disagreement. The terms "recommend" and "suggest" are used when the consensus was ≥70% and <70%, respectively.
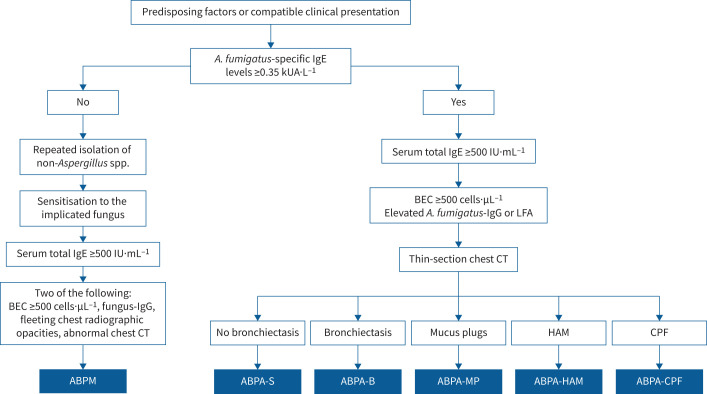
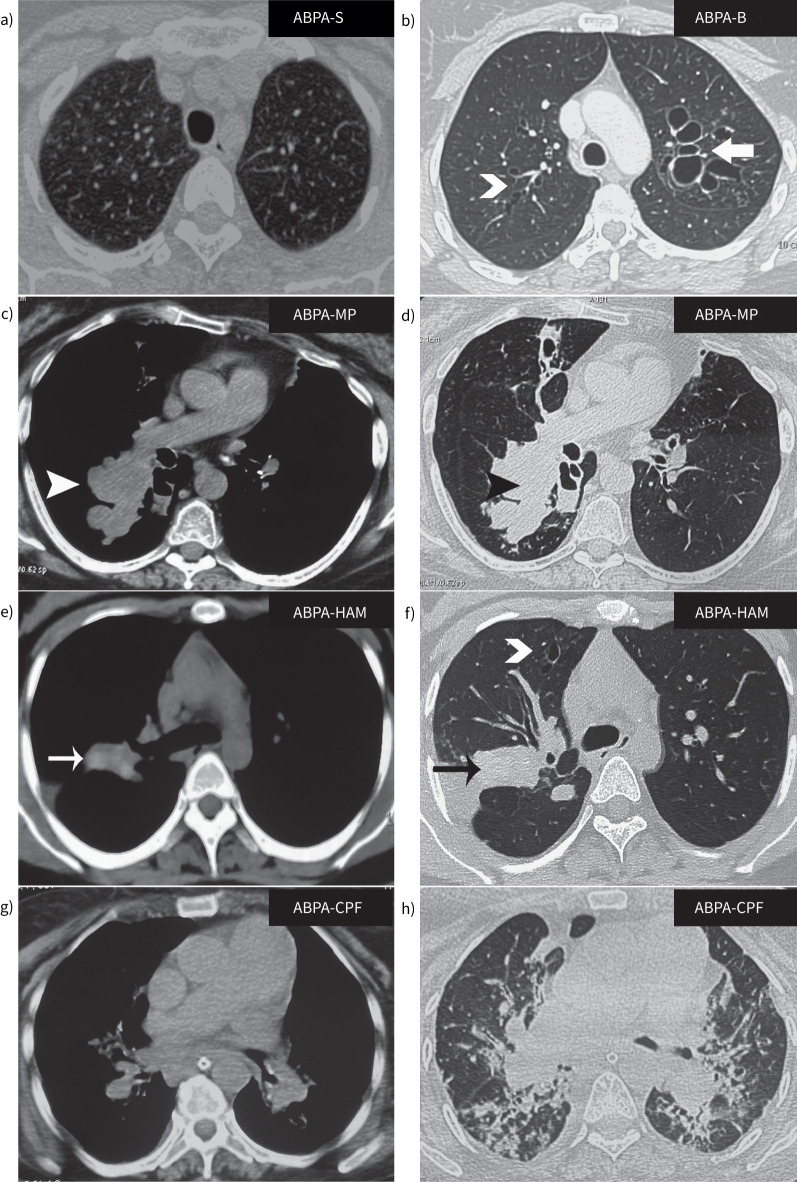
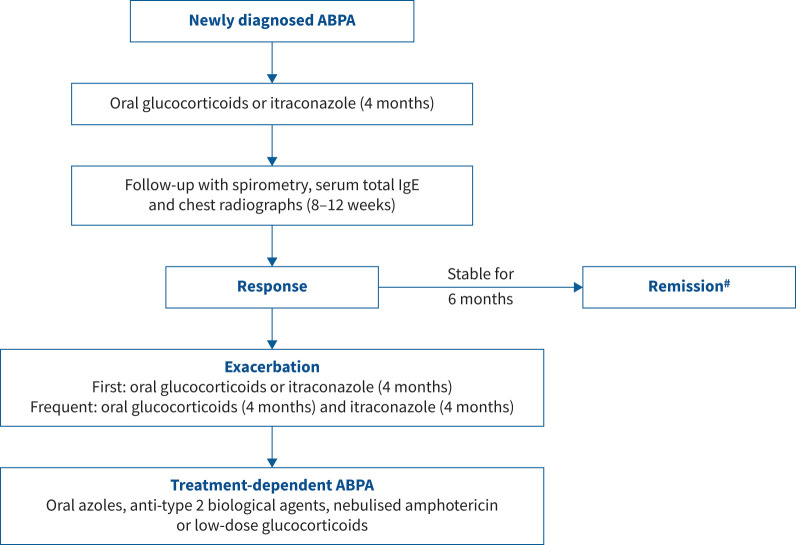
We recommend screening for sensitisation using fungus-specific IgE in all newly diagnosed asthmatic adults at tertiary care but only difficult-to-treat asthmatic children. We recommend diagnosing ABPA in those with predisposing conditions or compatible clinico-radiological presentation, with a mandatory demonstration of fungal sensitisation and serum total IgE ≥500 IU·mL and two of the following: fungal-specific IgG, peripheral blood eosinophilia or suggestive imaging. ABPM is considered in those with an ABPA-like presentation but normal -IgE. Additionally, diagnosing ABPM requires repeated growth of the causative fungus from sputum. We do not routinely recommend treating asymptomatic ABPA patients. We recommend oral prednisolone or itraconazole monotherapy for treating acute ABPA (newly diagnosed or exacerbation), with prednisolone and itraconazole combination only for treating recurrent ABPA exacerbations. We have devised an objective multidimensional criterion to assess treatment response.
We have framed consensus guidelines for diagnosing, classifying and treating ABPA/M for patient care and research.
国际人体与动物真菌学会(ISHAM)工作组十年前提出了治疗变应性支气管肺曲霉病(ABPA)的建议。由于诊断和治疗方法的进步,需要更新这些建议。
召集了一个国际专家小组,采用改良 Delphi 法(两轮在线和一轮面对面会议)制定成人和儿童 ABPA(由 spp.引起)和变应性支气管肺真菌病(ABPM;由 spp.以外的真菌引起)的管理指南。我们将共识定义为≥70%的同意或不同意。当共识≥70%和<70%时,分别使用“推荐”和“建议”这两个词。
我们建议在所有新诊断的三级保健成年哮喘患者中筛选真菌特异性 IgE 以筛查 过敏,但仅在治疗困难的哮喘儿童中筛选。我们建议在有易感条件或符合临床影像学表现的患者中诊断 ABPA,强制性地证明真菌过敏和血清总 IgE≥500 IU·mL-1 和以下两项:真菌特异性 IgG、外周血嗜酸性粒细胞增多或提示性影像学。在具有 ABPA 样表现但正常 IgE 的患者中考虑 ABPM。此外,诊断 ABPM 需要从痰液中反复培养出致病真菌。我们不常规建议治疗无症状 ABPA 患者。我们建议口服泼尼松龙或伊曲康唑单药治疗急性 ABPA(新诊断或恶化),仅在治疗复发性 ABPA 恶化时使用泼尼松龙和伊曲康唑联合治疗。我们制定了一个客观的多维标准来评估治疗反应。
我们为 ABPA/M 的诊断、分类和治疗制定了共识指南,以用于患者护理和研究。