Department of Anesthesiology and Pain Medicine, Seoul National University College of Medicine, Seoul Metropolitan Government Seoul National University Boramae Medical Center, 20, Boramae-ro 5-gil, Dongjak-gu, Seoul, 07061, Republic of Korea.
Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Gangnam Severance Hospital, 211, Eonju-ro, Gangnam-gu, Seoul, Republic of Korea.
Sci Rep. 2024 Feb 29;14(1):4980. doi: 10.1038/s41598-024-55537-0.
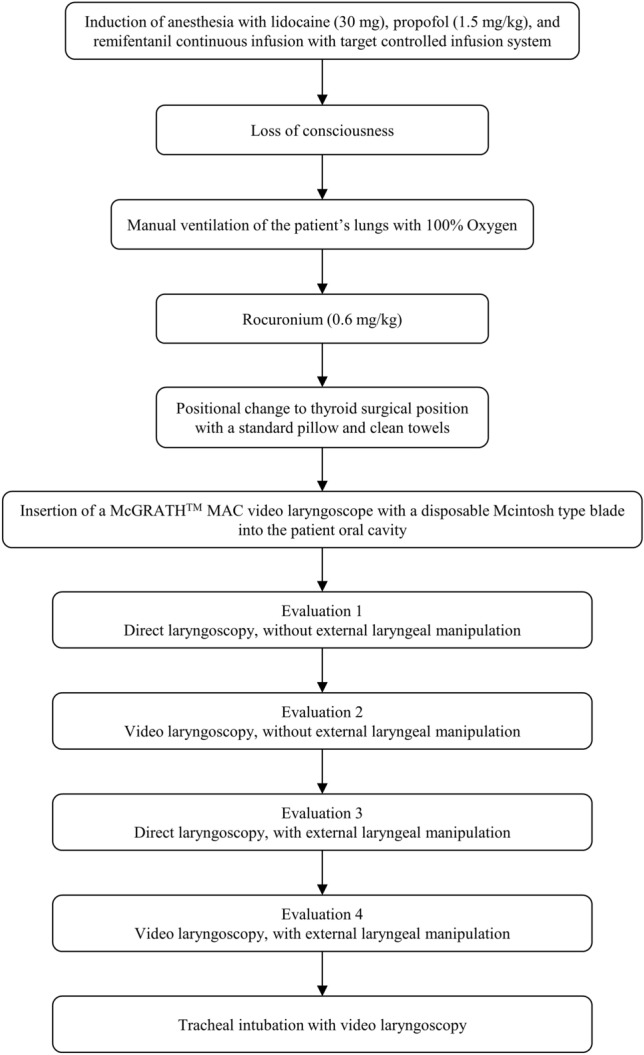
This observational study aimed to compare the glottic view between video and direct laryngoscopy for tracheal intubation in the surgical position for thyroid surgery with intraoperative neuromonitoring. Patients scheduled for elective thyroid surgery with intraoperative neuromonitoring were enrolled. After the induction of anesthesia, patients were positioned in the thyroid surgical posture with a standard inclined pillow under their head and back. An investigator assessed the glottic view using the percentage of glottic opening (POGO) scale and the modified Cormack-Lehane grade in direct laryngoscopy and then video laryngoscopy sequentially while using the same McGRATH™ MAC video laryngoscope at once, with or without external laryngeal manipulation, at the surgical position. A total of thirty-nine patients were participated in this study. Without external laryngeal manipulation, the POGO scale significantly improved during video laryngoscopy compared to direct laryngoscopy in the thyroid surgical position (60.0 ± 38.2% vs. 22.4 ± 23.8%; mean difference (MD) 37.6%, 95% confidence interval (CI) = [29.1, 46.0], P < 0.001). Additionally, with external laryngeal manipulation, the POGO scale showed a significant improvement during video laryngoscopy compared to direct laryngoscopy (84.6 ± 22.9% vs. 58.0 ± 36.3%; MD 26.7%, 95% CI = [18.4, 35.0] (P < 0.001). The superiority of video laryngoscopy was also observed for the modified Cormack-Lehane grade. In conclusion, video laryngoscopy with the McGRATH™ MAC video laryngoscope, when compared to direct laryngoscopy with it, improved the glottic view during tracheal intubation in the thyroid surgical position. This enhancement may potentially facilitate the proper placement of the electromyography tracheal tube and prevent tube displacement due to positional change for thyroid surgery.
这项观察性研究旨在比较视频喉镜和直接喉镜在甲状腺手术中经皮神经监测的手术体位下进行气管插管的声门显露情况。研究纳入了择期行甲状腺手术并接受术中神经监测的患者。在全身麻醉诱导后,患者采用标准的头高脚低位并在头背部下方垫一个倾斜枕。由一名研究人员使用声门显露百分比(POGO)量表和改良 Cormack-Lehane 分级评估直接喉镜和视频喉镜下的声门显露情况,然后在手术体位下同时使用同一种 McGRATH™ MAC 视频喉镜进行评估,评估时是否行外部喉镜施压。共有 39 例患者参与了这项研究。在手术体位下,不进行外部喉镜施压时,视频喉镜下的 POGO 量表评分显著优于直接喉镜(60.0 ± 38.2%比 22.4 ± 23.8%;平均差值(MD)37.6%,95%置信区间(CI)为[29.1,46.0],P < 0.001)。此外,进行外部喉镜施压时,视频喉镜下的 POGO 量表评分也显著优于直接喉镜(84.6 ± 22.9%比 58.0 ± 36.3%;MD 26.7%,95% CI 为[18.4,35.0],P < 0.001)。改良 Cormack-Lehane 分级也显示出了视频喉镜的优势。总之,与直接喉镜相比,McGRATH™ MAC 视频喉镜在甲状腺手术体位下进行气管插管时可改善声门显露情况。这种改善可能有助于正确放置肌电图监测气管导管,并防止因甲状腺手术而改变体位导致的导管移位。