Department of Otorhinolaryngology, Head and Neck Surgery, University Medical Center Groningen, University of Groningen, Hanzeplein 1, P.O. Box 30 001, 9700 RB, Groningen, The Netherlands.
Department of Epidemiology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Eur Arch Otorhinolaryngol. 2024 May;281(5):2619-2626. doi: 10.1007/s00405-024-08528-w. Epub 2024 Mar 1.
To identify associations between frailty and non-response to follow-up questionnaires, in a longitudinal head and neck cancer (HNC) study with patient-reported outcome measures (PROMs).
Patients referred with HNC were included in OncoLifeS, a prospective data-biobank, underwent Geriatric Assessment (GA) and frailty screening ahead of treatment, and were followed up at 3, 6, 12 and 24 months after treatment using the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 and Head and Neck 35. Statistical analysis for factors associated with non-response was done using Generalized Linear Mixed Models.
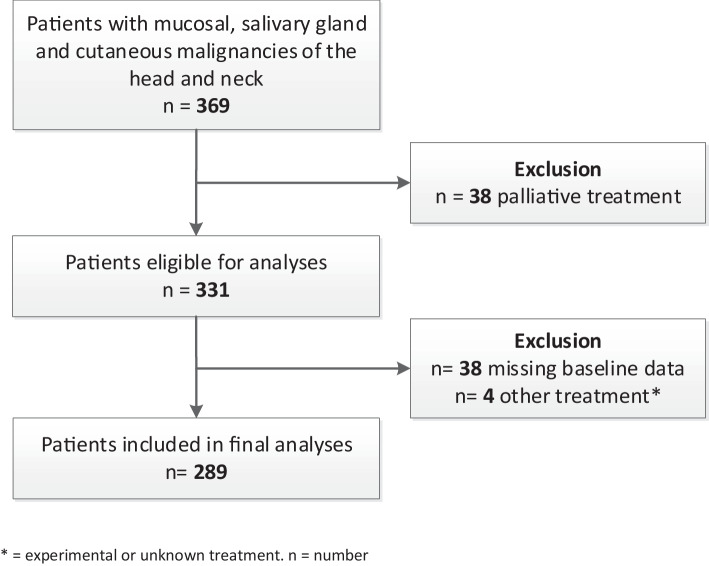
289 patients were eligible for analysis. Mean age was 68.4 years and 68.5% were male. Restrictions in Activities of Daily Living [OR 4.46 (2.04-9.78)] and Instrumental Activities of Daily Living [OR 4.33 (2.27-8.24)], impaired mobility on Timed Up and Go test [OR 3.95 (1.85-8.45)], cognitive decline [OR 4.85 (2.28-10.35)] and assisted living (OR 5.54 (2.63-11.67)] were significantly associated with non-response. Frailty screening, with Geriatric 8 and Groningen Frailty Indicator, was also associated with non-response [OR, respectively, 2.64 (1.51-4.59) and 2.52 (1.44-4.44)]. All findings remained significant when adjusted for other factors that were significantly associated with non-response, such as higher age, longer study duration and subsequent death.
Frail HNC patients respond significantly worse to follow-up PROMs. The drop-out and underrepresentation of frail patients in studies may lead to attrition bias, and as a result underestimating the effect sizes of associations. This is of importance when handling and interpreting such data.
在一项使用患者报告结局测量(PROM)的头颈部癌症(HNC)纵向研究中,确定脆弱与随访问卷无应答之间的关联。
将被转诊为 HNC 的患者纳入 OncoLifeS 前瞻性数据生物库中,在治疗前进行老年评估(GA)和虚弱筛查,并在治疗后 3、6、12 和 24 个月使用欧洲癌症研究与治疗组织生活质量问卷核心 30 项和头颈部 35 项进行随访。使用广义线性混合模型对与无应答相关的因素进行统计分析。
289 名患者符合分析条件。平均年龄为 68.4 岁,68.5%为男性。日常生活活动受限[OR 4.46(2.04-9.78)]和工具性日常生活活动受限[OR 4.33(2.27-8.24)]、计时起立行走测试中行动不便[OR 3.95(1.85-8.45)]、认知功能下降[OR 4.85(2.28-10.35)]和辅助生活[OR 5.54(2.63-11.67)]与无应答显著相关。使用老年 8 项和格罗宁根虚弱指标进行的虚弱筛查也与无应答相关[OR 分别为 2.64(1.51-4.59)和 2.52(1.44-4.44)]。当调整与无应答显著相关的其他因素(如年龄较大、研究持续时间较长和随后死亡)时,所有发现仍然具有统计学意义。
虚弱的 HNC 患者对随访 PROM 的反应明显较差。在研究中,虚弱患者的脱落和代表性不足可能导致损耗偏差,从而低估关联的效应大小。在处理和解释此类数据时,这一点很重要。