Department of Radiology, Charité-Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Hindenburgdamm 30, 12203, Berlin, Germany.
Academic Department of Diagnostic and Interventional Radiology and Paediatric Radiology, Protestant Hospital of the Bethel Foundation, Bielefeld University, Medical School and University Medical Center East Westphalia-Lippe, Burgsteig 13, 33617, Bielefeld, Germany.
Sci Rep. 2024 Mar 5;14(1):5379. doi: 10.1038/s41598-024-55821-z.
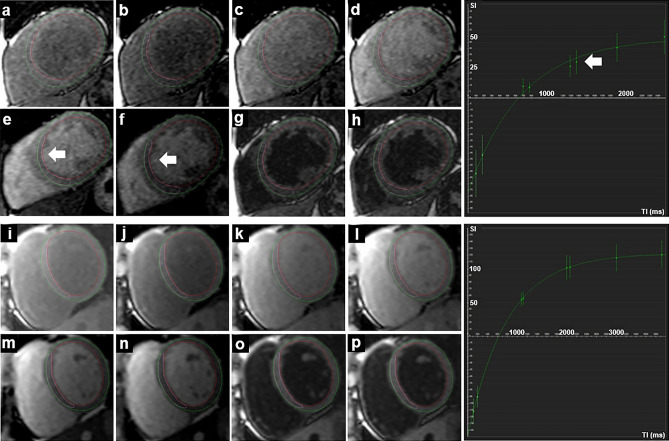
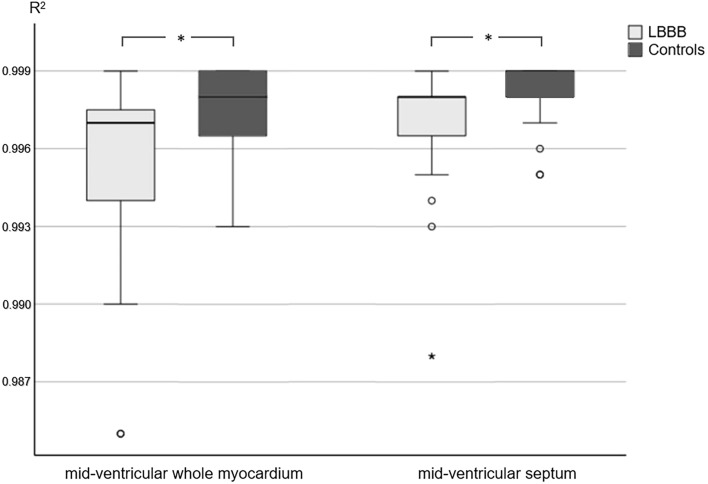
Tissue characterisation using T1 mapping has become an established magnetic resonance imaging (MRI) technique to detect myocardial diseases. This retrospective study aimed to determine the influence of left bundle branch block (LBBB) on T1 mapping at 1.5 T. Datasets of 36 patients with LBBB and 27 healthy controls with T1 mapping (Modified Look-Locker inversion-recovery (MOLLI), 5(3)3 sampling) were included. T1 relaxation times were determined on mid-cavity short-axis images. R maps were generated as a pixel-wise indicator for the goodness of the fit of T1 maps. R values were significantly lower in patients with LBBB than in healthy controls (whole myocardium/septum, 0.997, IQR, 0.00 vs. 0.998, IQR, 0.00; p = 0.008/0.998, IQR, 0.00 vs. 0.999, IQR, 0.00; p = 0.027). Manual correction of semi-automated evaluation tended to improve R values but not significantly. Strain analysis was performed and the systolic dyssynchrony index (SDI) was calculated as a measure for left ventricular dyssynchrony. While MRI is generally prone to artefacts, lower goodness of the fit in LBBB may be mainly attributable to asynchronous contraction. Therefore, careful checking of the source data and, if necessary, manual post-processing is important. New techniques might improve the goodness of the fit of T1 mapping by reducing sampling in the motion prone diastole of LBBB patients.
使用 T1 映射进行组织特征分析已经成为一种成熟的磁共振成像 (MRI) 技术,可用于检测心肌疾病。本回顾性研究旨在确定左束支传导阻滞 (LBBB) 对 1.5T 下 T1 映射的影响。研究纳入了 36 例 LBBB 患者和 27 例健康对照者的 T1 映射数据集(改良 Look-Locker 反转恢复 (MOLLI),5(3)3 采样)。在心脏中部短轴图像上确定 T1 弛豫时间。R 图作为 T1 图拟合好坏的像素级指示生成。LBBB 患者的 R 值明显低于健康对照组(整个心肌/室间隔,0.997,IQR,0.00 与 0.998,IQR,0.00;p=0.008/0.998,IQR,0.00 与 0.999,IQR,0.00;p=0.027)。半自动评估的手动校正倾向于提高 R 值,但没有统计学意义。进行应变分析,并计算左心室不同步指数 (SDI) 作为左心室不同步的度量。虽然 MRI 通常容易出现伪影,但 LBBB 下拟合度较差可能主要归因于收缩不同步。因此,仔细检查原始数据,如果有必要,进行手动后处理非常重要。新技术可能通过减少 LBBB 患者易受运动影响的舒张期采样来提高 T1 映射的拟合度。