Pandanaboyana Sanjay, Knoph Cecilie Siggaard, Olesen Søren Schou, Jones Michael, Lucocq James, Samanta Jayanta, Talukdar Rupjyoti, Capurso Gabriele, de-Madaria Enrique, Yadav Dhiraj, Siriwardena Ajith K, Windsor John, Drewes Asbjørn Mohr, Nayar Manu
HPB and Transplant Unit, Freeman Hospital, Newcastle Upon Tyne, UK.
Population Health Sciences Institute, Newcastle University, Newcastle Upon Tyne, UK.
United European Gastroenterol J. 2024 Apr;12(3):326-338. doi: 10.1002/ueg2.12542. Epub 2024 Mar 4.
The effect of analgesic modalities on short-term outcomes in acute pancreatitis remains unknown. However, preclinical models have raised safety concerns regarding opioid use in patients with acute pancreatitis.
This study aimed to assess the association between analgesics, particularly opioids, and severity and mortality in hospitalised patients with acute pancreatitis.
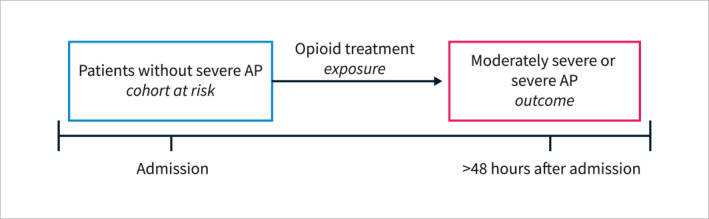
This prospective multicentre cohort study recruited consecutive patients admitted with a first episode of acute pancreatitis between April 1 and 30 June 2022, with a 1-month follow-up. Data on aetiology, clinical course, and analgesic treatment were collected. The primary outcome was the association between opioid analgesia and acute pancreatitis severity, which was analysed using univariate and multivariate analyses.
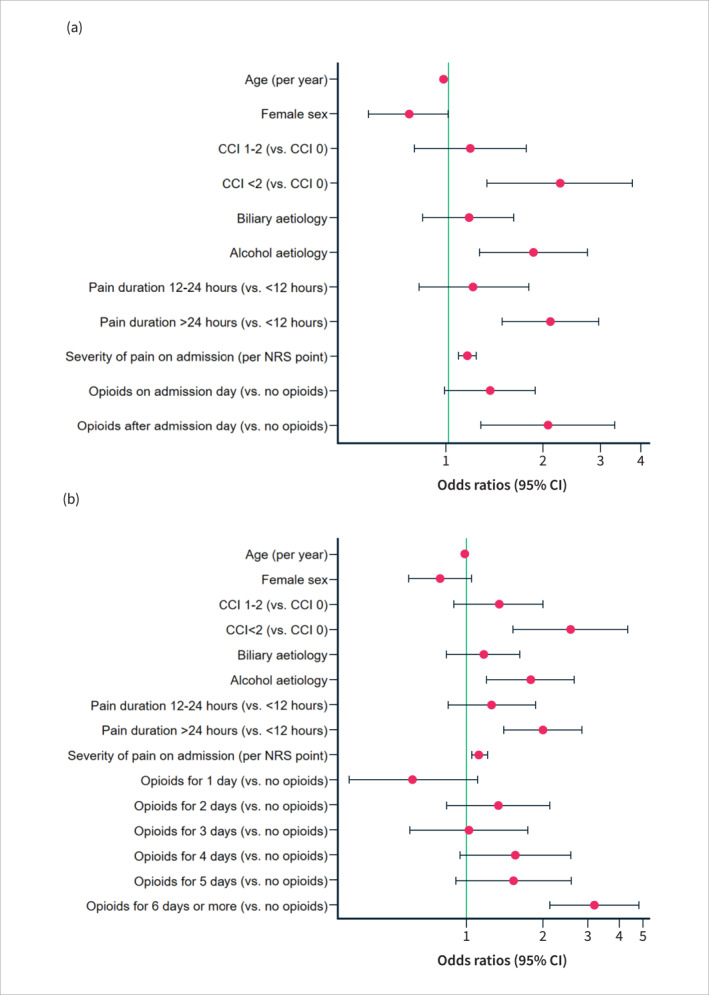
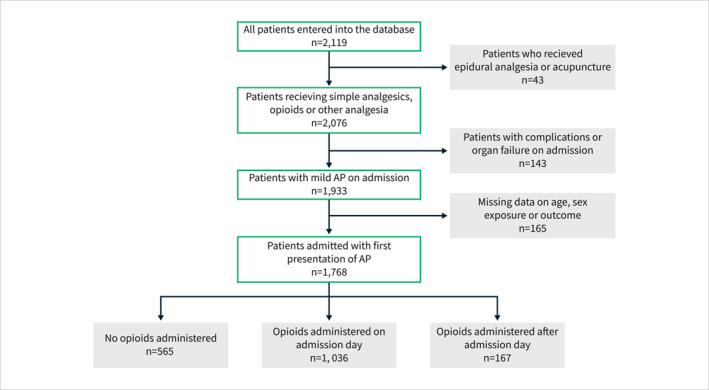
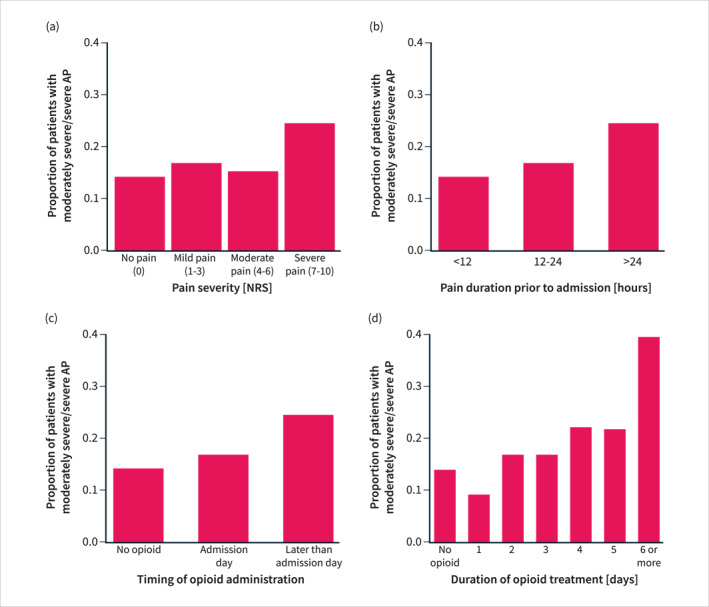
Among a total of 1768 patients, included from 118 centres across 27 countries, 1036 (59%) had opioids administered on admission day, and 167 (9%) received opioids after admission day. On univariate analysis, moderately severe or severe acute pancreatitis was associated with male sex, Asian ethnicity, alcohol aetiology, comorbidity, predicted severe acute pancreatitis, higher pain scores, longer pain duration and opioid treatment (all p < 0.001). On multivariate analysis, comorbidity, alcohol aetiology, longer pain duration and higher pain scores increased the risk of moderately severe or severe acute pancreatitis (all p < 0.001). Furthermore, opioids administered after admission day (but not on admission day) doubled the risk of moderately severe or severe disease (OR 2.07 (95% CI, 1.29-3.33); p = 0.003). Opioid treatment for 6 days or more was an independent risk factor for moderately severe or severe acute pancreatitis (OR 3.21 (95% CI, 2.16-4.79; p < 0.001). On univariate analysis, longer opioid duration was associated with mortality.
Opioid treatment increased the risk of more severe acute pancreatitis only when administered after admission day or for 6 days or more. Future randomised studies should re-evaluate whether opioids might be safe in acute pancreatitis.
镇痛方式对急性胰腺炎短期预后的影响尚不清楚。然而,临床前模型引发了对急性胰腺炎患者使用阿片类药物安全性的担忧。
本研究旨在评估镇痛药,尤其是阿片类药物,与住院急性胰腺炎患者的严重程度和死亡率之间的关联。
这项前瞻性多中心队列研究纳入了2022年4月1日至6月30日期间因首次急性胰腺炎发作而连续入院的患者,并进行了1个月的随访。收集了病因、临床病程和镇痛治疗的数据。主要结局是阿片类镇痛与急性胰腺炎严重程度之间的关联,采用单因素和多因素分析进行分析。
在来自27个国家118个中心的总共1768例患者中,1036例(59%)在入院当天接受了阿片类药物治疗,167例(9%)在入院当天之后接受了阿片类药物治疗。单因素分析显示,中度严重或重度急性胰腺炎与男性、亚洲种族、酒精性病因、合并症、预测的重度急性胰腺炎、更高的疼痛评分、更长的疼痛持续时间和阿片类药物治疗相关(所有p<0.001)。多因素分析显示,合并症、酒精性病因、更长的疼痛持续时间和更高的疼痛评分增加了中度严重或重度急性胰腺炎的风险(所有p<0.001)。此外,入院当天之后(而非入院当天)使用阿片类药物使中度严重或重度疾病的风险增加了一倍(比值比2.07(95%置信区间,1.29-3.33);p=0.003)。使用阿片类药物6天或更长时间是中度严重或重度急性胰腺炎的独立危险因素(比值比3.21(95%置信区间,2.16-4.79;p<0.001)。单因素分析显示,更长的阿片类药物使用时间与死亡率相关。
仅在入院当天之后或使用6天或更长时间时,阿片类药物治疗会增加更严重急性胰腺炎的风险。未来的随机研究应重新评估阿片类药物在急性胰腺炎中是否可能安全。