Lee Seungbaek, Arffman Riikka K, Komsi Elina K, Lindgren Outi, Kemppainen Janette, Kask Keiu, Saare Merli, Salumets Andres, Piltonen Terhi T
Department of Obstetrics and Gynaecology, Research Unit of Clinical Medicine, Medical Research Center, Oulu University Hospital, University of Oulu, Oulu 90220, Finland.
Department of Obstetrics and Gynaecology, Institute of Clinical Medicine, University of Tartu, Tartu 50406, Estonia.
J Pathol Inform. 2024 Feb 1;15:100364. doi: 10.1016/j.jpi.2024.100364. eCollection 2024 Dec.
The human endometrium undergoes a monthly cycle of tissue growth and degeneration. During the mid-secretory phase, the endometrium establishes an optimal niche for embryo implantation by regulating cellular composition (e.g., epithelial and stromal cells) and differentiation. Impaired endometrial development observed in conditions such as polycystic ovary syndrome (PCOS) and recurrent implantation failure (RIF) contributes to infertility. Surprisingly, despite the importance of the endometrial lining properly developing prior to pregnancy, precise measures of endometrial cellular composition in these two infertility-associated conditions are entirely lacking. Additionally, current methods for measuring the epithelial and stromal area have limitations, including intra- and inter-observer variability and efficiency.
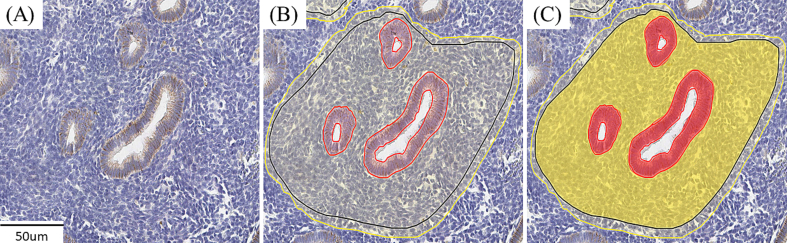
We utilized a deep-learning artificial intelligence (AI) model, created on a cloud-based platform and developed in our previous study. The AI model underwent training to segment both areas populated by epithelial and stromal endometrial cells. During the training step, a total of 28.36 mm2 areas were annotated, comprising 2.56 mm2 of epithelium and 24.87 mm2 of stroma. Two experienced pathologists validated the performance of the AI model. 73 endometrial samples from healthy control women were included in the sample set to establish cycle phase-dependent dynamics of the endometrial epithelial-to-stroma ratio from the proliferative (PE) to secretory (SE) phases. In addition, 91 samples from PCOS cases, accounting for the presence or absence of ovulation and representing all menstrual cycle phases, and 29 samples from RIF patients on day 5 after progesterone administration in the hormone replacement treatment cycle were also included and analyzed in terms of cellular composition.
Our AI model exhibited reliable and reproducible performance in delineating epithelial and stromal compartments, achieving an accuracy of 92.40% and 99.23%, respectively. Moreover, the performance of the AI model was comparable to the pathologists' assessment, with F1 scores exceeding 82% for the epithelium and >96% for the stroma. Next, we compared the endometrial epithelial-to-stromal ratio during the menstrual cycle in women with PCOS and in relation to endometrial receptivity status in RIF patients. The ovulatory PCOS endometrium exhibited epithelial cell proportions similar to those of control and healthy women's samples in every cycle phase, from the PE to the late SE, correlating with progesterone levels (control SE, r2 = 0.64, FDR < 0.001; PCOS SE, r2 = 0.52, FDR < 0.001). The mid-SE endometrium showed the highest epithelial percentage compared to both the early and late SE endometrium in both healthy women and PCOS patients. Anovulatory PCOS cases showed epithelial cellular fractions comparable to those of PCOS cases in the PE (Anovulatory, 14.54%; PCOS PE, 15.56%, p = 1.00). We did not observe significant differences in the epithelial-to-stroma ratio in the hormone-induced endometrium in RIF patients with different receptivity statuses.
The AI model rapidly and accurately identifies endometrial histology features by calculating areas occupied by epithelial and stromal cells. The AI model demonstrates changes in epithelial cellular proportions according to the menstrual cycle phase and reveals no changes in epithelial cellular proportions based on PCOS and RIF conditions. In conclusion, the AI model can potentially improve endometrial histology assessment by accelerating the analysis of the cellular composition of the tissue and by ensuring maximal objectivity for research and clinical purposes.
人类子宫内膜经历每月一次的组织生长和退化周期。在分泌中期,子宫内膜通过调节细胞组成(如上皮细胞和基质细胞)和分化,为胚胎着床建立最佳微环境。在多囊卵巢综合征(PCOS)和反复着床失败(RIF)等情况下观察到的子宫内膜发育受损会导致不孕。令人惊讶的是,尽管子宫内膜在怀孕前正常发育很重要,但在这两种与不孕相关的情况下,完全缺乏对子宫内膜细胞组成的精确测量方法。此外,目前测量上皮和基质面积的方法存在局限性,包括观察者内和观察者间的变异性以及效率问题。
我们利用了一个基于深度学习的人工智能(AI)模型,该模型在基于云的平台上创建,并在我们之前的研究中开发。该AI模型经过训练,以分割由上皮和基质子宫内膜细胞占据的区域。在训练步骤中,总共标注了28.36平方毫米的区域,其中包括2.56平方毫米的上皮和24.87平方毫米的基质。两名经验丰富的病理学家验证了AI模型的性能。样本集中包括73例来自健康对照女性的子宫内膜样本,以建立从增殖期(PE)到分泌期(SE)子宫内膜上皮与基质比例的周期阶段依赖性动态变化。此外,还纳入了91例PCOS病例的样本,这些样本考虑了排卵情况并代表了所有月经周期阶段,以及29例在激素替代治疗周期中孕激素给药后第5天的RIF患者样本,并对其细胞组成进行了分析。
我们的AI模型在描绘上皮和基质区域方面表现出可靠且可重复的性能,上皮区域和基质区域的准确率分别达到92.40%和99.23%。此外,AI模型的性能与病理学家的评估相当,上皮区域的F1分数超过82%,基质区域的F1分数大于96%。接下来,我们比较了PCOS女性月经周期中的子宫内膜上皮与基质比例以及RIF患者中与子宫内膜接受性状态相关的比例。排卵型PCOS子宫内膜在从PE到晚期SE的每个周期阶段,其上皮细胞比例与对照和健康女性样本相似,与孕激素水平相关(对照SE,r2 = 0.64,FDR < 0.001;PCOS SE,r2 = 0.52,FDR < 0.001)。与健康女性和PCOS患者的早期和晚期SE子宫内膜相比,中期SE子宫内膜的上皮百分比最高。无排卵型PCOS病例的上皮细胞分数与PE期的PCOS病例相当(无排卵型,14.54%;PCOS PE,15.56%,p = 1.00)。我们在不同接受性状态的RIF患者的激素诱导子宫内膜中未观察到上皮与基质比例的显著差异。
AI模型通过计算上皮和基质细胞占据的面积,快速准确地识别子宫内膜组织学特征。AI模型展示了上皮细胞比例根据月经周期阶段的变化,并且未显示基于PCOS和RIF情况的上皮细胞比例变化。总之,AI模型通过加速组织细胞组成分析并确保研究和临床目的的最大客观性,有可能改善子宫内膜组织学评估。