Cardiocentro Ticino Institute, Ente Ospedaliero Cantonale, Via Tesserete 48, CH-6900 Lugano, Switzerland.
Hôpital Cardiologique du Haut-Lévêque, CHU Bordeaux, L'Institut de Rythmologie et modélisation Cardiaque (LIRYC), Université Bordeaux, Bordeaux, France.
Eur Heart J. 2024 Apr 7;45(14):1255-1265. doi: 10.1093/eurheartj/ehae133.
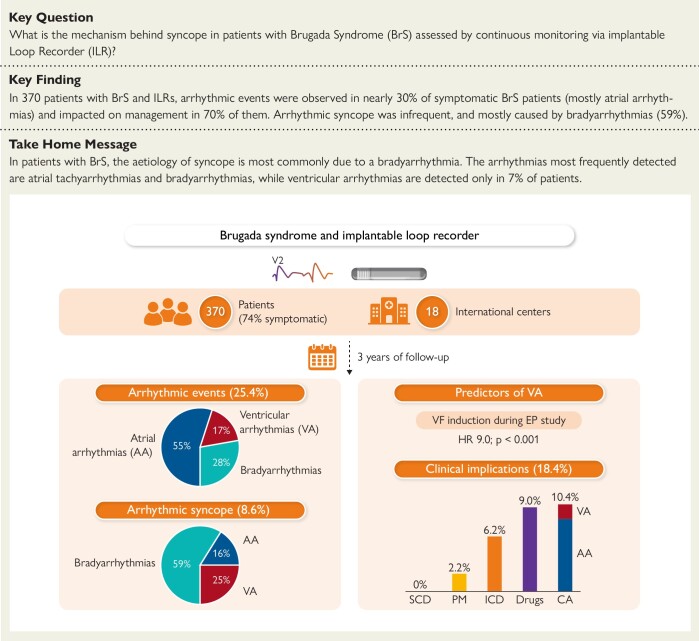
Available data on continuous rhythm monitoring by implantable loop recorders (ILRs) in patients with Brugada syndrome (BrS) are scarce. The aim of this multi-centre study was to evaluate the diagnostic yield and clinical implication of a continuous rhythm monitoring strategy by ILRs in a large cohort of BrS patients and to assess the precise arrhythmic cause of syncopal episodes.
A total of 370 patients with BrS and ILRs (mean age 43.5 ± 15.9, 33.8% female, 74.1% symptomatic) from 18 international centers were included. Patients were followed with continuous rhythm monitoring for a median follow-up of 3 years.
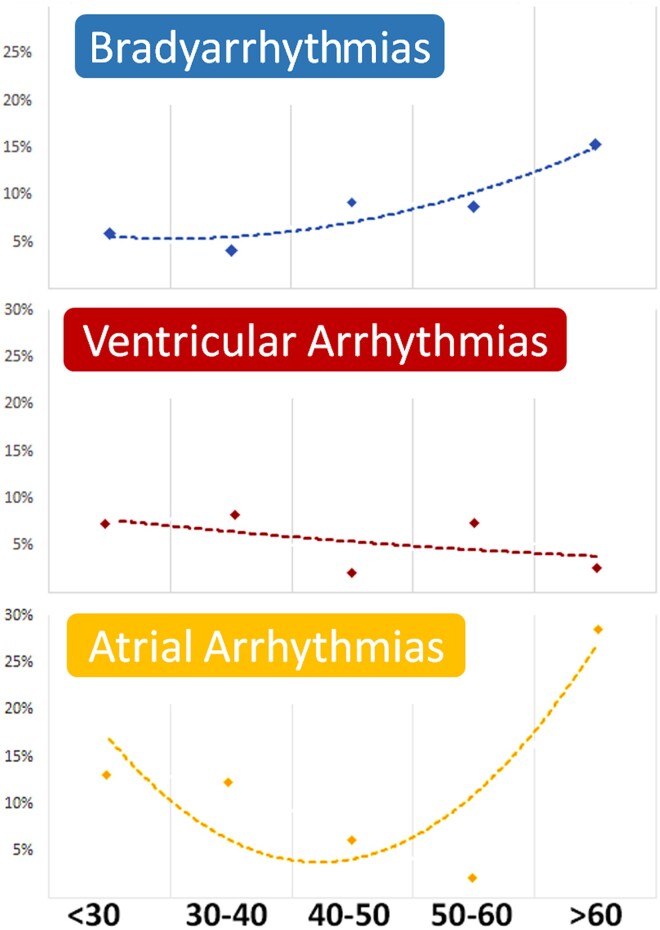
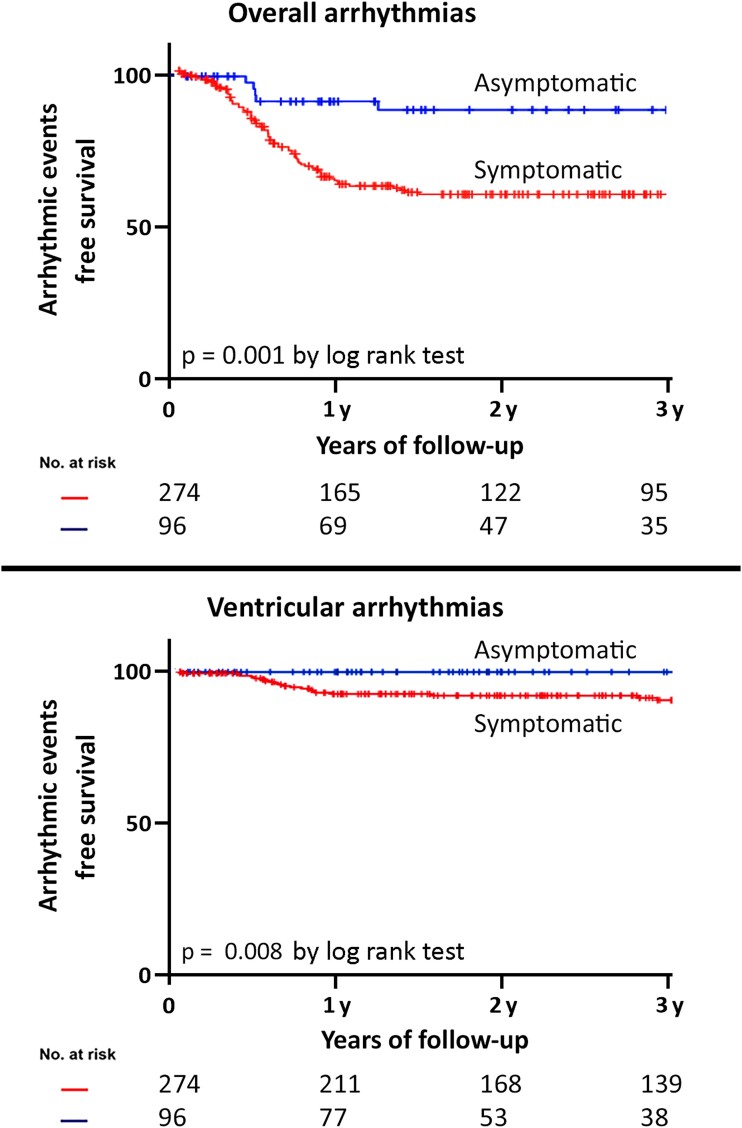
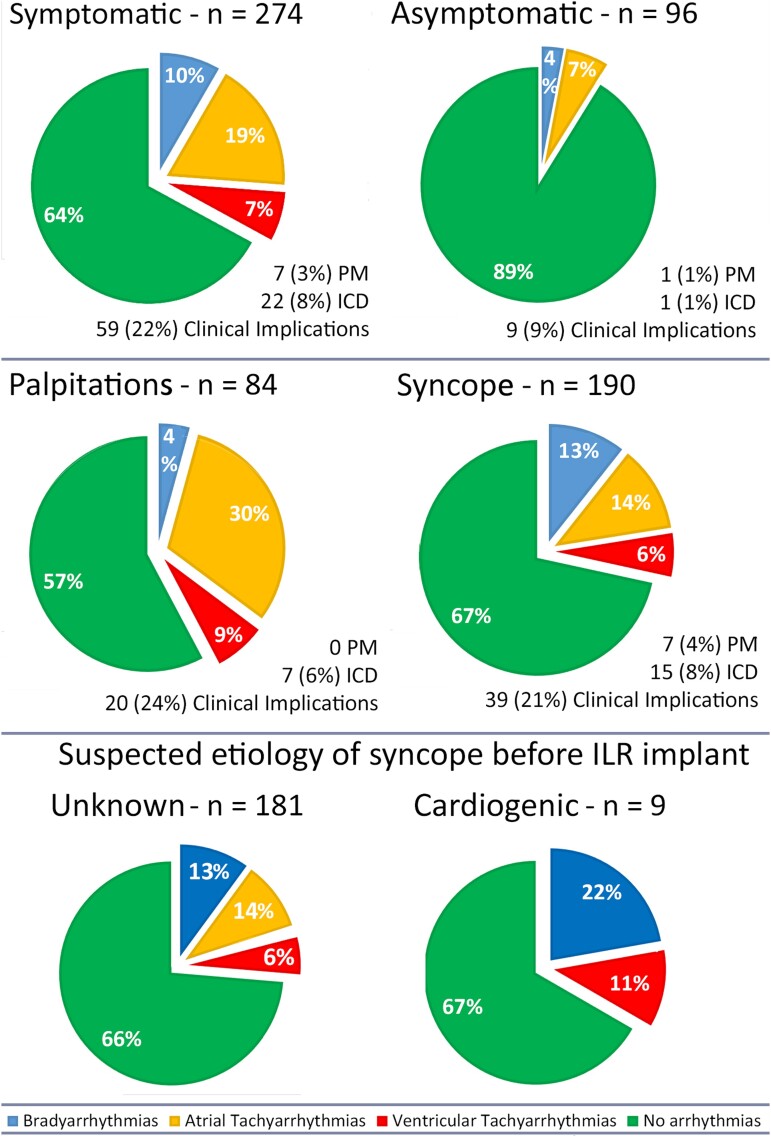
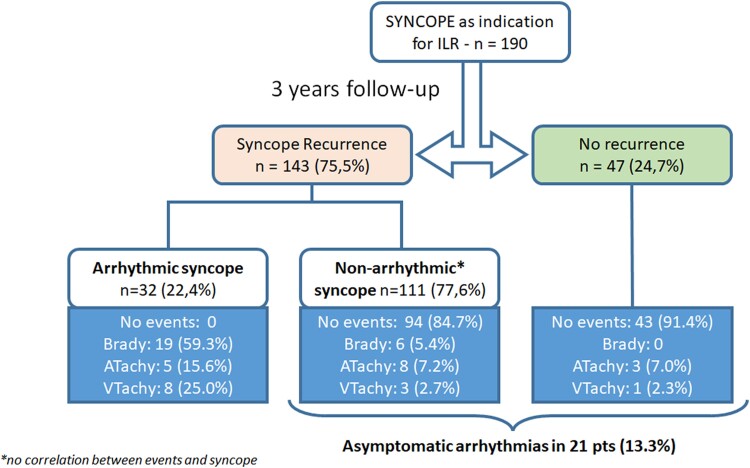
During follow-up, an arrhythmic event was recorded in 30.7% of symptomatic patients [18.6% atrial arrhythmias (AAs), 10.2% bradyarrhythmias (BAs), and 7.3% ventricular arrhythmias (VAs)]. In patients with recurrent syncope, the aetiology was arrhythmic in 22.4% (59.3% BAs, 25.0% VAs, and 15.6% AAs). The ILR led to drug therapy initiation in 11.4%, ablation procedure in 10.9%, implantation of a pacemaker in 2.5%, and a cardioverter-defibrillator in 8%. At multivariate analysis, the presence of symptoms [hazard ratio (HR) 2.5, P = .001] and age >50 years (HR 1.7, P = .016) were independent predictors of arrhythmic events, while inducibility of ventricular fibrillation at the electrophysiological study (HR 9.0, P < .001) was a predictor of VAs.
ILR detects arrhythmic events in nearly 30% of symptomatic BrS patients, leading to appropriate therapy in 70% of them. The most commonly detected arrhythmias are AAs and BAs, while VAs are detected only in 7% of cases. Symptom status can be used to guide ILR implantation.
目前关于植入式循环记录仪(ILR)在 Brugada 综合征(BrS)患者中连续节律监测的可用数据较少。本多中心研究的目的是评估 ILR 在大量 BrS 患者中的连续节律监测策略的诊断效果和临床意义,并评估晕厥发作的确切心律失常原因。
共纳入来自 18 个国际中心的 370 例 BrS 患者和 ILR(平均年龄 43.5±15.9 岁,33.8%为女性,74.1%有症状)。患者接受中位数为 3 年的连续节律监测随访。
随访期间,有症状患者中 30.7%(18.6%房性心律失常[AA]、10.2%缓率失常[BA]和 7.3%室性心律失常[VA])记录到心律失常事件。在有反复晕厥的患者中,病因是心律失常的占 22.4%(59.3%BA、25.0%VA 和 15.6%AA)。ILR 导致 11.4%患者开始药物治疗、10.9%患者接受消融术、2.5%患者植入起搏器、8%患者植入除颤器。多变量分析显示,有症状(危险比[HR] 2.5,P=.001)和年龄>50 岁(HR 1.7,P=.016)是心律失常事件的独立预测因素,而电生理研究时可诱发性室颤(HR 9.0,P<.001)是 VA 的预测因素。
ILR 可检测出近 30%有症状 BrS 患者的心律失常事件,其中 70%患者接受了适当的治疗。最常见的心律失常是 AA 和 BA,而仅在 7%的病例中检测到 VA。症状状态可用于指导 ILR 植入。