Division of Pulmonology, Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Republic of Korea.
Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, 50-1 Yonsei-ro, Seodaemun-gu, Seoul, 03722, Republic of Korea.
Respir Res. 2024 Mar 7;25(1):112. doi: 10.1186/s12931-024-02730-4.
Whether COVID-19-induced acute respiratory distress syndrome (ARDS) should be approached differently in terms of mechanical ventilation therapy compared to other virus-induced ARDS is debatable. Therefore, we aimed to ascertain whether the respiratory mechanical characteristics of COVID-19-induced ARDS differ from those of influenza A induced ARDS, in order to establish a rationale for mechanical ventilation therapy in COVID-19-induced ARDS.
This was a retrospective cohort study comparing patients with COVID-19-induced ARDS and influenza A induced ARDS. We included intensive care unit (ICU) patients with COVID-19 or Influenza A aged ≥ 19, who were diagnosed with ARDS according to the Berlin definition between January 2015 and July 2021. Ventilation parameters for respiratory mechanics were collected at specific times on days one, three, and seven after intubation.
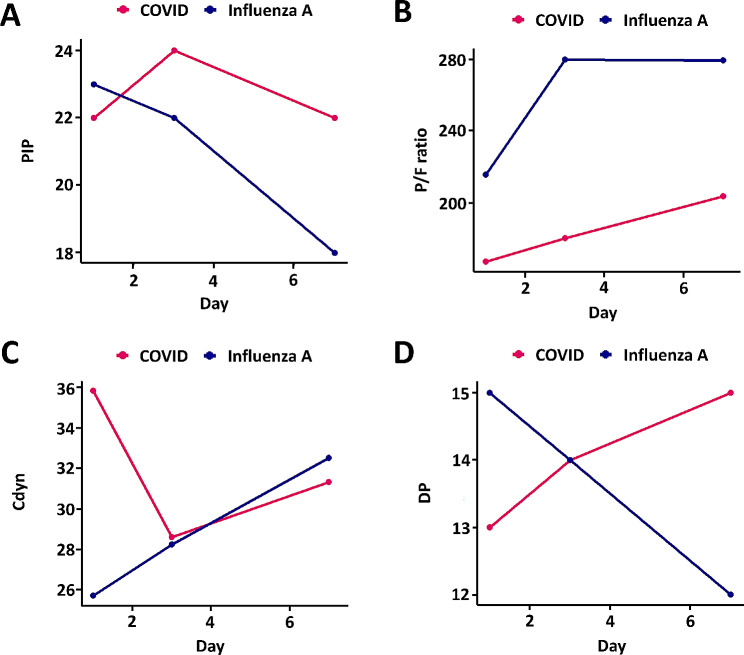
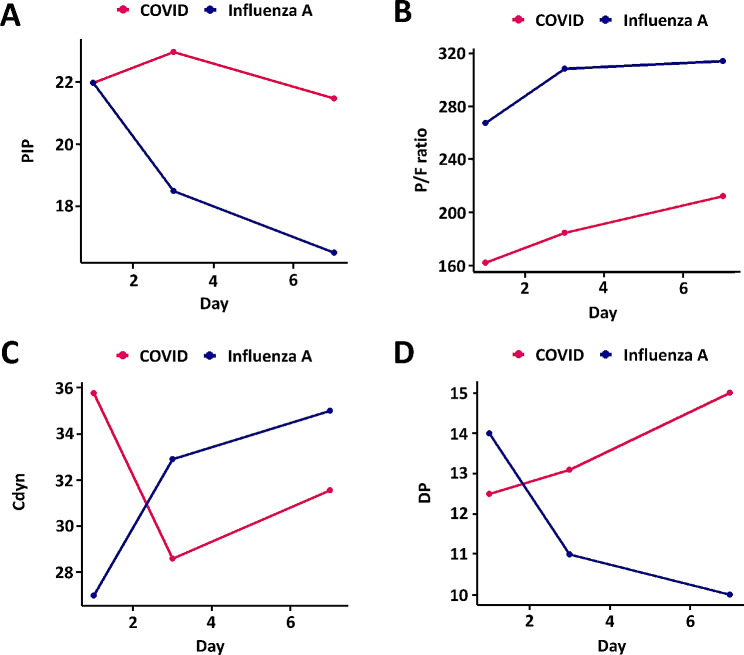
The median age of the 87 participants was 71.0 (62.0-78.0) years old, and 63.2% were male. The ratio of partial pressure of oxygen in arterial blood to the fractional of inspiratory oxygen concentration in COVID-19-induced ARDS was lower than that in influenza A induced ARDS during the initial stages of mechanical ventilation (influenza A induced ARDS 216.1 vs. COVID-19-induced ARDS 167.9, p = 0.009, day 1). The positive end expiratory pressure remained consistently higher in the COVID-19 group throughout the follow-up period (7.0 vs. 10.0, p < 0.001, day 1). COVID-19 and influenza A initially showed different directions for peak inspiratory pressure and dynamic compliance; however, after day 3, both groups exhibited similar directions. Dynamic driving pressure exhibited opposite trends between the two groups during mechanical ventilation.
Respiratory mechanics show clear differences between COVID-19-induced ARDS and influenza A induced ARDS. Based on these findings, we can consider future treatment strategies for COVID-19-induced ARDS.
与其他病毒引起的 ARDS 相比,COVID-19 引起的急性呼吸窘迫综合征(ARDS)在机械通气治疗方面是否应该有所不同,这是有争议的。因此,我们旨在确定 COVID-19 引起的 ARDS 的呼吸力学特征是否与流感 A 引起的 ARDS 不同,以便为 COVID-19 引起的 ARDS 的机械通气治疗建立依据。
这是一项回顾性队列研究,比较了 COVID-19 引起的 ARDS 患者和流感 A 引起的 ARDS 患者。我们纳入了年龄≥19 岁的 2015 年 1 月至 2021 年 7 月期间在 ICU 因 COVID-19 或流感 A 而诊断为 ARDS 的患者。在插管后第 1、3 和 7 天收集特定时间的呼吸力学通气参数。
87 名参与者的中位年龄为 71.0(62.0-78.0)岁,63.2%为男性。在机械通气的初始阶段,COVID-19 引起的 ARDS 患者的动脉血氧分压与吸入氧浓度的分数比值低于流感 A 引起的 ARDS(流感 A 引起的 ARDS 为 216.1,COVID-19 引起的 ARDS 为 167.9,p=0.009,第 1 天)。在整个随访期间,COVID-19 组的呼气末正压一直保持较高(第 1 天为 7.0,第 10.0,p<0.001)。COVID-19 和流感 A 最初在吸气峰压和动态顺应性方面表现出不同的方向;然而,在第 3 天后,两组均表现出相似的方向。在机械通气过程中,两组之间的动态驱动压表现出相反的趋势。
COVID-19 引起的 ARDS 和流感 A 引起的 ARDS 的呼吸力学表现出明显的差异。基于这些发现,我们可以考虑 COVID-19 引起的 ARDS 的未来治疗策略。