Liu Minghui, Wei Ning, Song Yuhu
Department of Gastroenterology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of Gastroenterology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430022, China.
Therap Adv Gastroenterol. 2024 Mar 4;17:17562848241234501. doi: 10.1177/17562848241234501. eCollection 2024.
Left-sided portal hypertension (LSPH) leads to life-threatening gastrointestinal (GI) bleeding. There are no recommendations or consensus about the management of GI bleeding caused by LSPH. This systematic review and meta-analysis were conducted to evaluate the incidence of GI bleeding and the mortality of patients with LSPH receiving different therapeutic strategies.
A systematic review and meta-analysis were performed to determine the efficacy of different therapeutic strategies for GI bleeding caused by LSPH.
All relevant studies were searched from PubMed, Embase, Web of Science, Cochrane Library, Scopus, ScienceDirect, MEDLINE, Google Scholar, CNKI, and Wanfang Data without language restriction through 15 November 2023. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated through RevMan5.3 software. (The Cochrane Collaboration, Copenhagen, Denmark).
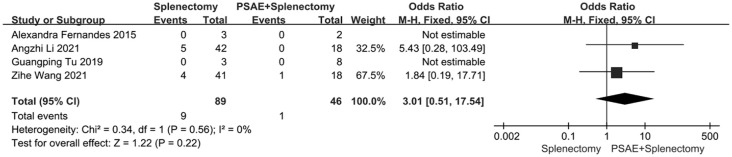
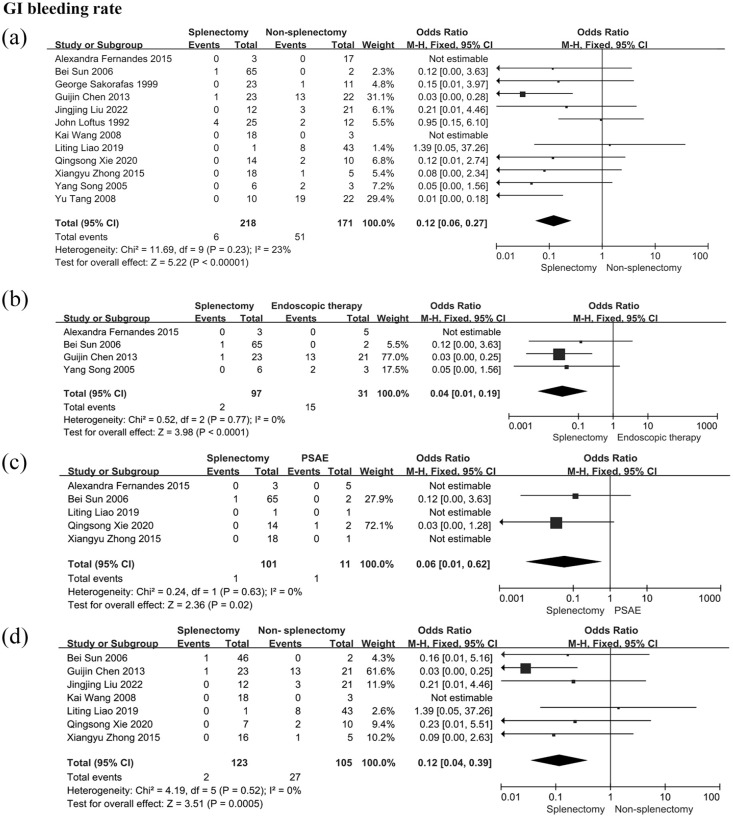
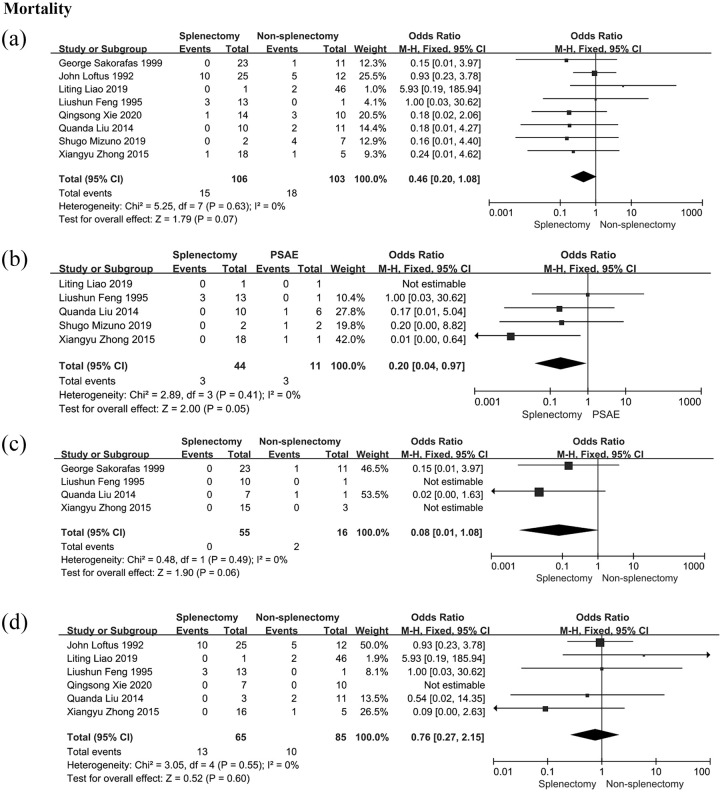
Seventeen retrospective studies and one prospective study involving 624 patients were included. This systematic review and meta-analysis found that: (1) splenectomy was more effective than non-splenectomy therapeutic strategies in reducing the incidence of GI bleeding caused by LSPH (OR: 0.12; 95% CI: 0.06-0.27); (2) splenectomy was superior to partial splenic artery embolism (PSAE) (OR: 0.06; 95% CI: 0.01-0.62) or endoscopic interventions (OR: 0.04; 95% CI: 0.01-0.19) in the prevention of GI bleeding, respectively; (3) no significant difference in the mortality was observed between splenectomy and non-splenectomy therapeutic strategies (OR: 0.46; 95% CI: 0.20-1.08); and (4) patients receiving preoperative PSAE followed by splenectomy had less intraoperative bleeding and shorter operative time than those receiving splenectomy.
This meta-analysis demonstrated that splenectomy is superior to non-splenectomy therapeutic strategies in reducing the incidence of GI bleeding from LSPH, which revealed that splenectomy should be recommended in the management of these patients.
This study has been registered on the PROSPERO database with the registration number CRD42023483764.
左侧门静脉高压(LSPH)可导致危及生命的胃肠道(GI)出血。目前对于LSPH所致GI出血的管理尚无推荐意见或共识。本系统评价和荟萃分析旨在评估接受不同治疗策略的LSPH患者GI出血的发生率和死亡率。
进行系统评价和荟萃分析,以确定不同治疗策略对LSPH所致GI出血的疗效。
通过检索PubMed、Embase、Web of Science、Cochrane图书馆、Scopus、ScienceDirect、MEDLINE、谷歌学术、中国知网和万方数据,收集截至2023年11月15日的所有相关研究,不限语言。通过RevMan5.3软件计算比值比(OR)和95%置信区间(CI)。(丹麦哥本哈根Cochrane协作网)。
纳入17项回顾性研究和1项前瞻性研究,共624例患者。本系统评价和荟萃分析发现:(1)在降低LSPH所致GI出血发生率方面,脾切除术比非脾切除术治疗策略更有效(OR:0.12;95%CI:0.06 - 0.27);(2)在预防GI出血方面,脾切除术分别优于部分脾动脉栓塞术(PSAE)(OR:0.06;95%CI:0.01 - 0.62)或内镜干预(OR:0.04;95%CI:0.01 - 0.19);(3)脾切除术和非脾切除术治疗策略在死亡率方面无显著差异(OR:0.46;95%CI:0.20 - 1.08);(4)术前接受PSAE然后行脾切除术的患者比单纯接受脾切除术的患者术中出血更少,手术时间更短。
本荟萃分析表明,在降低LSPH所致GI出血发生率方面,脾切除术优于非脾切除术治疗策略,这表明在这些患者的管理中应推荐脾切除术。
本研究已在PROSPERO数据库注册,注册号为CRD42023483764。