National Institute of Public Health, Ljubljana, Slovenia.
National Institute of Health, Environment and Food, Ljubljana, Slovenia.
Front Public Health. 2024 Feb 21;12:1294261. doi: 10.3389/fpubh.2024.1294261. eCollection 2024.
Despite decreasing COVID-19 disease severity during the Omicron waves, a proportion of patients still require hospitalization and intensive care.
To compare demographic characteristics, comorbidities, vaccination status, and previous infections in patients hospitalized for community-associated COVID-19 (CAC) in predominantly Delta, Omicron BA.1 and BA.4/5 SARS-CoV-2 waves.
Data were extracted from three national databases-the National COVID-19 Database, National Vaccination Registry and National Registry of Hospitalizations.
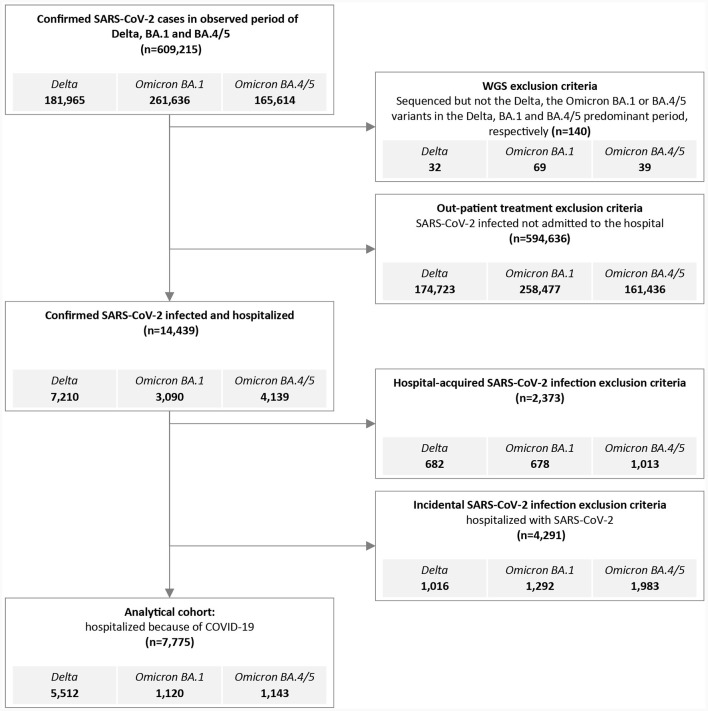
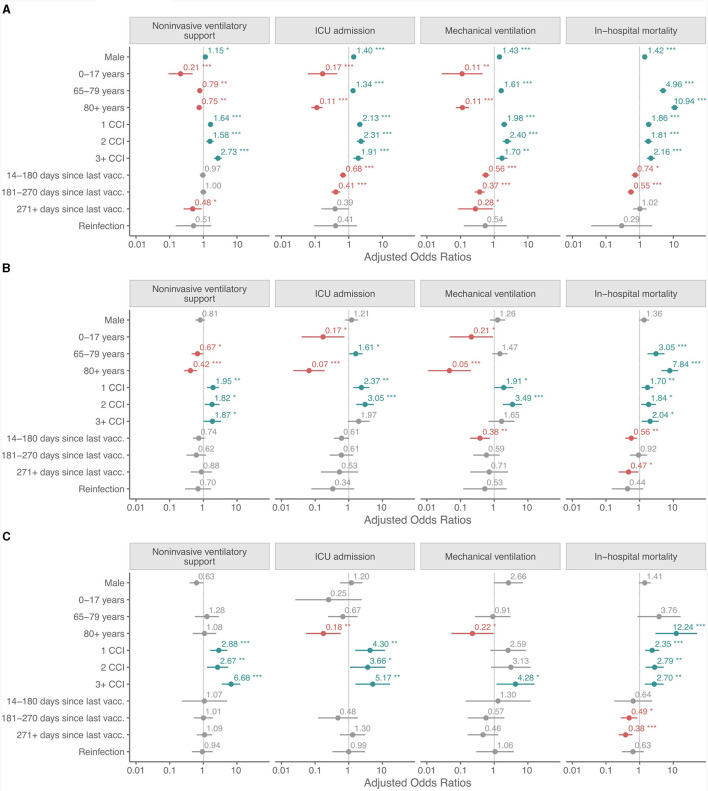
Among the hospitalized CAC patients analyzed in this study, 5,512 were infected with Delta, 1,120 with Omicron BA.1, and 1,143 with the Omicron BA.4/5 variant. The age and sex structure changed from Delta to BA.4/5, with the proportion of women (9.5% increase), children and adolescents (10.4% increase), and octa- and nonagenarians increasing significantly (24.5% increase). Significantly more patients had comorbidities (measured by the Charlson Comorbidity Index), 30.3% in Delta and 43% in BA.4/5 period. The need for non-invasive ventilatory support (NiVS), ICU admission, mechanical ventilation (MV), and in-hospital mortality (IHM) decreased from Delta to Omicron BA.4/5 period for 12.6, 13.5, 11.5, and 6.3%, respectively. Multivariate analysis revealed significantly lower odds for ICU admission (OR 0.68, CI 0.54-0.84, < 0.001) and IHM (OR 0.74, CI 0.58-0.93, = 0.011) during the Delta period in patients who had been fully vaccinated or boosted with a COVID-19 vaccine within the previous 6 months. In the BA.1 variant period, patients who had less than 6 months elapsed between the last vaccine dose and SARS-CoV-2 positivity had lower odds for MV (OR 0.38, CI 0.18-0.72, = 0.005) and IHM (OR 0.56, CI 0.37- 0.83, = 0.005), but not for NIVS or ICU admission.
The likelihood of developing severe CAC in hospitalized patients was higher in those with the Delta and Omicron BA.1 variant compared to BA.4/5.
尽管奥密克戎(Omicron)浪潮期间 COVID-19 疾病严重程度有所下降,但仍有一部分患者需要住院治疗和接受重症监护。
比较主要为德尔塔(Delta)、奥密克戎 BA.1 和 BA.4/5 变异株引起的社区获得性 COVID-19(CAC)住院患者的人口统计学特征、合并症、疫苗接种情况和既往感染情况。
数据来自三个国家数据库-国家 COVID-19 数据库、国家疫苗接种登记处和国家住院登记处。
在本研究分析的 CAC 住院患者中,5512 例感染了德尔塔,1120 例感染了奥密克戎 BA.1,1143 例感染了奥密克戎 BA.4/5 变异株。从德尔塔到 BA.4/5,年龄和性别结构发生了变化,女性比例(增加 9.5%)、儿童和青少年(增加 10.4%)以及 80 岁以上和 90 岁以上人群的比例显著增加(增加 24.5%)。有合并症(以 Charlson 合并症指数衡量)的患者明显增多,Delta 时期为 30.3%,BA.4/5 时期为 43%。与 Delta 时期相比,需要无创通气支持(NiVS)、入住 ICU、机械通气(MV)和院内死亡率(IHM)的患者比例在奥密克戎 BA.4/5 时期分别降低了 12.6%、13.5%、11.5%和 6.3%。多变量分析显示,在完全接种 COVID-19 疫苗或在过去 6 个月内加强接种疫苗的患者中,Delta 时期 ICU 入住(OR 0.68,CI 0.54-0.84, < 0.001)和 IHM(OR 0.74,CI 0.58-0.93, = 0.011)的可能性显著降低。在 BA.1 变异株时期,最后一剂疫苗和 SARS-CoV-2 阳性之间间隔不到 6 个月的患者,MV(OR 0.38,CI 0.18-0.72, = 0.005)和 IHM(OR 0.56,CI 0.37-0.83, = 0.005)的可能性降低,但 NiVS 和 ICU 入住的可能性没有降低。
与 BA.4/5 相比,Delta 和奥密克戎 BA.1 变异株引起的住院 CAC 患者发生严重 CAC 的可能性更高。