Department of Internal Medicine, Hospital Universitario Ramón y Cajal, IRYCIS, Madrid, Spain.
Department of Medicine and Medical Specialties, Facultad de Medicina y Ciencias de la Salud, Universidad de Alcalá, IRYCIS, Madrid, Spain.
ESC Heart Fail. 2024 Jun;11(3):1739-1747. doi: 10.1002/ehf2.14749. Epub 2024 Mar 7.
The current literature provides limited guidance on the best diuretic strategy post-hospitalization for acute heart failure (AHF). It is postulated that the efficacy and safety of the outpatient diuretic regimen may be significantly influenced by the degree of fluid overload (FO) encountered during hospitalization. We hypothesize that in patients with more pronounced FO, reducing their regular oral diuretic dosage might be associated with an elevated risk of unfavourable clinical outcomes.
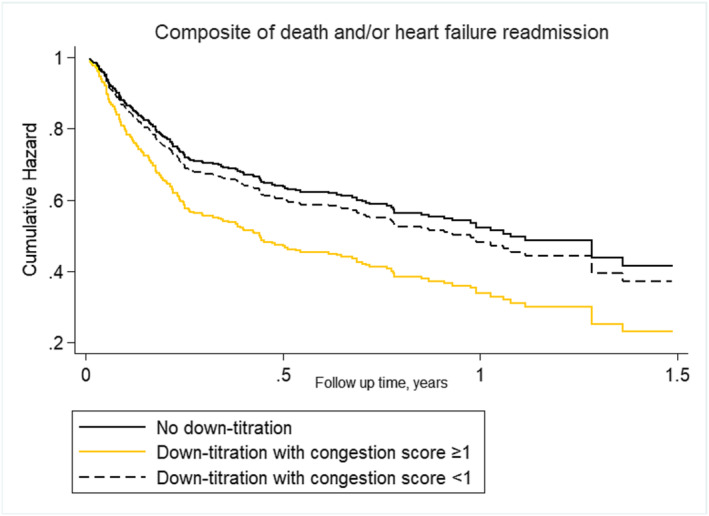
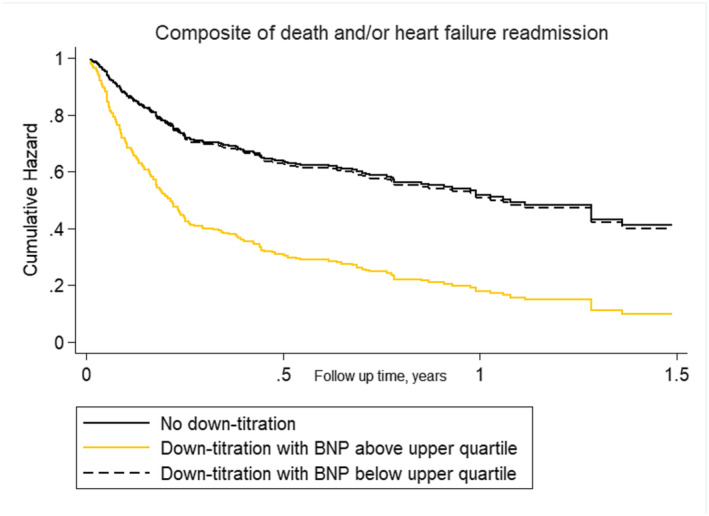
It was a retrospective observational study of 410 patients hospitalized for AHF in which the dose of furosemide at admission and discharge was collected. Patients were categorized across diuretic dose status into two groups: (i) the down-titration group and (ii) the stable/up-titration group. FO status was evaluated by a clinical congestion score and circulating biomarkers. The endpoint of interest was the composite of time to all-cause death and/or heart failure readmission. A multivariable Cox proportional hazard regression model was constructed to analyse the endpoints. The median age was 86 (78-92) years, 256 (62%) were women, and 80% had heart failure with preserved ejection fraction. After multivariate adjustment, the down-titration furosemide equivalent dose remained not associated with the risk of the combined endpoint in the whole sample (hazard ratio 1.34, 95% confidence interval 0.86-2.06, P = 0.184). The risk of the combination of death and/or worsening heart failure associated with the diuretic strategy at discharge was significantly influenced by FO status, including clinical congestion scores and circulating proxies of FO like BNP and cancer antigen 125.
In patients hospitalized for AHF, furosemide down-titration does not imply an increased risk of mortality and/or heart failure readmission. However, FO status modifies the effect of down-titration on the outcome. In patients with severe congestion or residual congestion at discharge, down-titration was associated with an increased risk of mortality and/or heart failure readmission.
目前的文献对急性心力衰竭(AHF)出院后最佳利尿剂策略提供的指导有限。据推测,门诊利尿剂方案的疗效和安全性可能会受到住院期间液体超负荷(FO)程度的显著影响。我们假设,在 FO 更明显的患者中,减少其常规口服利尿剂剂量可能与不良临床结局的风险升高相关。
这是一项对 410 例因 AHF 住院的患者进行的回顾性观察性研究,其中收集了入院时和出院时呋塞米的剂量。根据利尿剂剂量状态将患者分为两组:(i)滴定剂量降低组和(ii)稳定/滴定剂量增加组。通过临床充血评分和循环生物标志物评估 FO 状态。感兴趣的终点是全因死亡和/或心力衰竭再入院的复合终点。构建多变量 Cox 比例风险回归模型来分析终点。中位年龄为 86(78-92)岁,256 例(62%)为女性,80%有射血分数保留的心力衰竭。经过多变量调整后,在整个样本中,滴定剂量降低的呋塞米等效剂量与复合终点的风险无相关性(危险比 1.34,95%置信区间 0.86-2.06,P=0.184)。出院时利尿剂策略与死亡和/或心力衰竭恶化相关的组合风险,FO 状态(包括临床充血评分和 FO 的循环标志物,如 BNP 和癌抗原 125)显著影响。
在因 AHF 住院的患者中,呋塞米剂量降低并不意味着死亡率和/或心力衰竭再入院的风险增加。然而,FO 状态改变了滴定剂量对结局的影响。在出院时充血严重或仍有充血的患者中,剂量降低与死亡率和/或心力衰竭再入院的风险增加相关。