Bone Marrow Transplantation Center, The First Affiliated Hospital, Zhejiang University School of Medicine, No. 79 Qingchun road, Hangzhou, 310003, China.
Department of Hematology, Ningbo Medical Treatment Center Li Huili Hospital, Ningbo, 315000, China.
Target Oncol. 2024 Mar;19(2):237-249. doi: 10.1007/s11523-024-01039-y. Epub 2024 Mar 11.
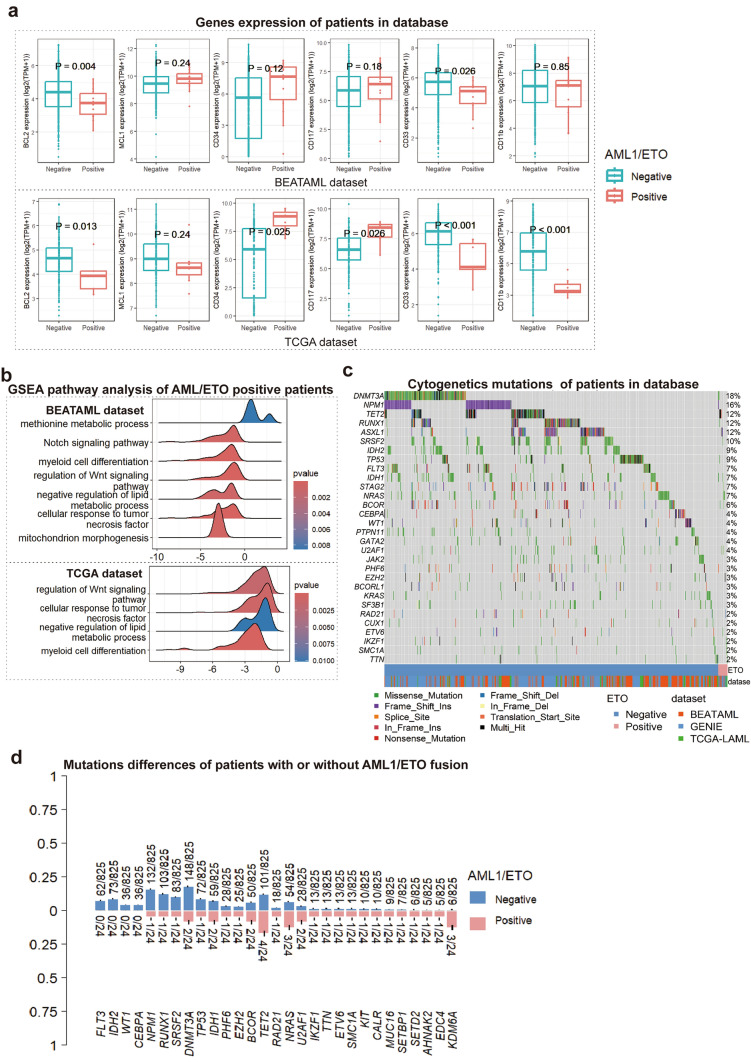
AML1/ETO fusion confers favorable prognosis in acute myeloid leukemia (AML) treated with intensive chemotherapy (IC). However, the impact of AML1/ETO fusion on the efficacy of venetoclax in the treatment of AML is unclear.
The aim of this study was to evaluate the efficacy of venetoclax plus hypomethylating agents (VEN/HMAs) in patients with AML1/ETO-positive AML.
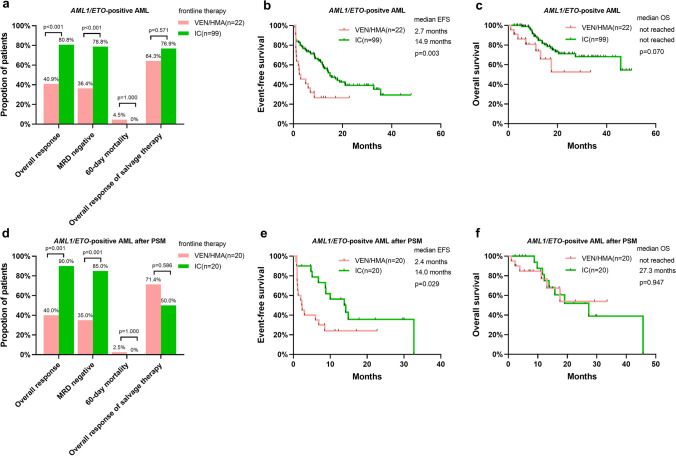
Patients with newly diagnosed AML in two centers were reviewed and divided into three cohorts: AML1/ETO-positive AML treated with frontline VEN/HMA (Cohort A), AML1/ETO-negative AML treated with frontline VEN/HMA (Cohort B), or AML1/ETO-positive AML treated with frontline IC (Cohort C). The response and survival were compared between the cohorts.
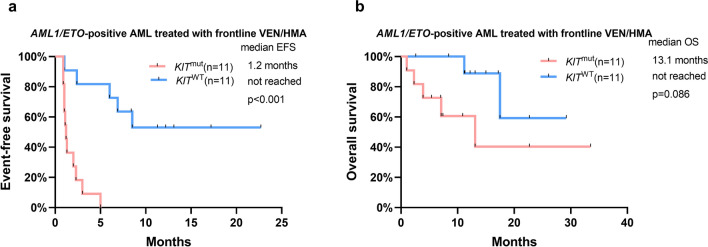
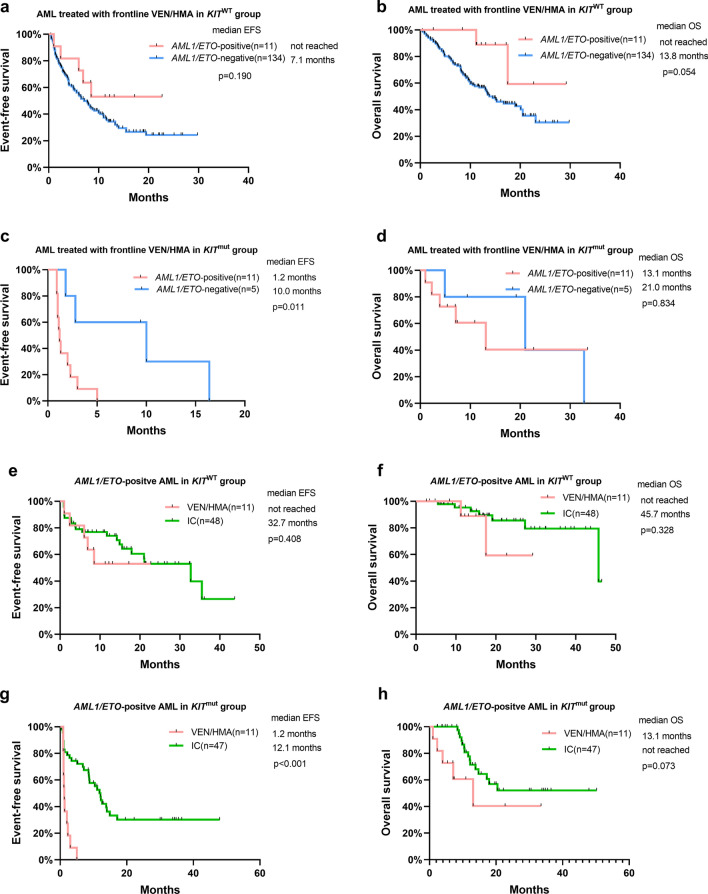
A total of 260 patients were included in the study. Patients in Cohort A had a significantly lower overall response rate (ORR) than patients in Cohort B (40.9% vs 71.2%, p = 0.005). The median event-free survival (EFS) in Cohort A and Cohort B was 2.7 months and 7.7 months, respectively, with no significant difference. The ORR and median EFS in Cohort C were 80.8% and 14.9 months, respectively, which were significantly superior to those in Cohort A, and the advantages remained significant after propensity score matching. ORR and EFS in KIT-mutated patients with AML1/ETO-positive AML receiving VEN/HMA were much inferior to those in KIT wild-type patients (ORR 0.0% vs 81.8%, p = 0.001; EFS 1.2 months vs not reached, p < 0.001).
Newly diagnosed AML patients with AML1/ETO fusion had a poor response to frontline VEN/HMA treatment. When determining induction therapy for patients with AML1/ETO-positive AML, IC should be preferred over VEN/HM.
AML1/ETO 融合在接受强化化疗(IC)治疗的急性髓系白血病(AML)中提供有利的预后。然而,AML1/ETO 融合对 venetoclax 治疗 AML 的疗效的影响尚不清楚。
本研究旨在评估 venetoclax 联合低甲基化剂(VEN/HMAs)在 AML1/ETO 阳性 AML 患者中的疗效。
对两个中心新诊断的 AML 患者进行了回顾性分析,并分为三组:一线接受 VEN/HMA 治疗的 AML1/ETO 阳性 AML 患者(A 组)、一线接受 VEN/HMA 治疗的 AML1/ETO 阴性 AML 患者(B 组)或一线接受 IC 治疗的 AML1/ETO 阳性 AML 患者(C 组)。比较了三组之间的反应和生存情况。
共纳入 260 例患者。A 组患者的总缓解率(ORR)明显低于 B 组(40.9% vs 71.2%,p=0.005)。A 组和 B 组的中位无事件生存(EFS)分别为 2.7 个月和 7.7 个月,无显著差异。C 组的 ORR 和中位 EFS 分别为 80.8%和 14.9 个月,明显优于 A 组,且经倾向评分匹配后优势仍显著。接受 VEN/HMA 治疗的 AML1/ETO 阳性伴 KIT 突变的 AML 患者的 ORR 和 EFS 明显低于 KIT 野生型患者(ORR 0.0% vs 81.8%,p=0.001;EFS 1.2 个月 vs 未达到,p<0.001)。
新诊断的 AML1/ETO 融合阳性 AML 患者对一线 VEN/HMA 治疗反应不佳。在为 AML1/ETO 阳性 AML 患者确定诱导治疗时,IC 应优先于 VEN/HM。