Key Laboratory of Environment and Health, Ministry of Education and Ministry of Environmental Protection, Department of Epidemiology and Biostatistics, School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
J Cachexia Sarcopenia Muscle. 2024 Jun;15(3):897-906. doi: 10.1002/jcsm.13447. Epub 2024 Mar 11.
Systemic inflammation and frailty have been implicated in osteoporosis (OP) and fracture risks; however, existing evidence remains limited and inconclusive. This study aimed to assess the associations of systemic inflammation and frailty phenotype with incident OP and fracture and to evaluate the mediating role of frailty phenotype.
The present study analysed data from the UK Biobank, a comprehensive and representative dataset encompassing over 500 000 individuals from the general population. Baseline peripheral blood cell counts were employed to calculate the systemic inflammation markers, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and systemic immune-inflammation index (SII). Frailty phenotype was assessed using five criteria, defined as frail (≥3 items met), pre-frail (1-2 items met) and non-frail (0 items met). OP and fracture events were confirmed through participants' health-related records. Multivariable linear and Cox regression models were utilized, along with mediation analysis.
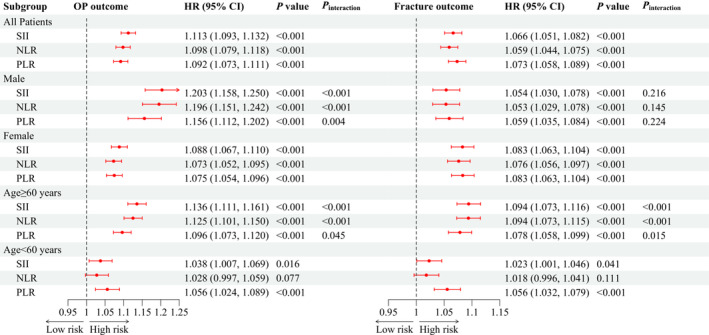
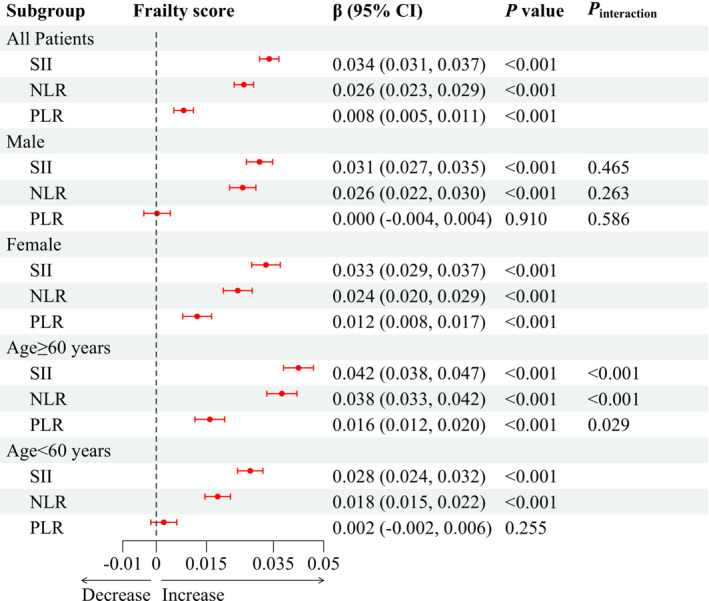
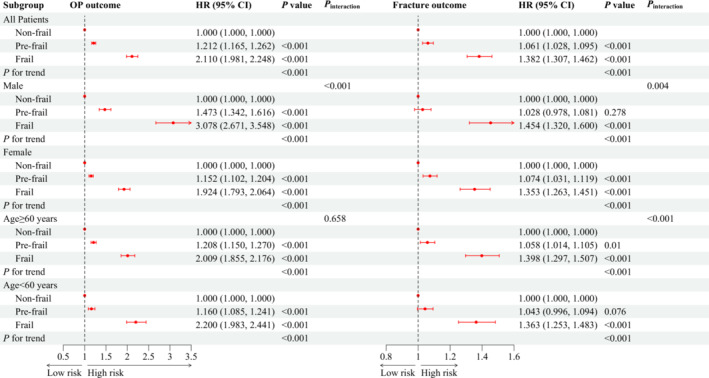
Increased systemic inflammation was associated with increased risks of OP and fracture. The corresponding hazard ratios and 95% confidence intervals (CIs) for OP risk per standard deviation increase in the log-transformed NLR, PLR and SII were 1.113 (1.093-1.132), 1.098 (1.079-1.118) and 1.092 (1.073-1.111), and for fracture risk, they were 1.066 (1.051-1.082), 1.059 (1.044-1.075) and 1.073 (1.058-1.089), respectively. Compared with the non-frail individuals, the pre-frail and frail ones showed an elevated OP risk by 21.2% (95% CI: 16.5-26.2%) and 111.0% (95% CI: 98.1-124.8%), respectively, and an elevated fracture risk by 6.1% (95% CI: 2.8-9.5%) and 38.2% (95% CI: 30.7-46.2%), respectively. The systemic inflammation level demonstrated a positive association with frailty, with β (95% CI) of 0.034 (0.031-0.037), 0.026 (0.023-0.029) and 0.008 (0.005-0.011) in response to per standard deviation increment in log-transformed SII, NLR and PLR, respectively. The frailty phenotype mediated the association between systemic inflammation and OP/fracture risk. Subgroup and sensitivity analyses confirmed the robustness of these findings.
Systemic inflammation and frailty phenotype are independently linked to increased risks of OP and fracture. The frailty phenotype partially mediates the association between systemic inflammation and osteoporotic traits. These results highlight the significance of interventions targeting systemic inflammation and frailty in OP and fracture prevention and management.
系统性炎症和衰弱与骨质疏松症(OP)和骨折风险有关;然而,现有证据仍然有限且不一致。本研究旨在评估系统性炎症和衰弱表型与 OP 和骨折事件的相关性,并评估衰弱表型的中介作用。
本研究分析了英国生物库的数据,该数据库是一个全面且具有代表性的数据集,包含来自普通人群的超过 50 万人的数据。使用基线外周血细胞计数来计算系统性炎症标志物,包括中性粒细胞与淋巴细胞比值(NLR)、血小板与淋巴细胞比值(PLR)和系统性免疫炎症指数(SII)。使用五个标准评估衰弱表型,定义为衰弱(≥3 项符合)、衰弱前期(1-2 项符合)和非衰弱(0 项符合)。通过参与者的健康相关记录来确认 OP 和骨折事件。使用多变量线性和 Cox 回归模型以及中介分析。
系统性炎症增加与 OP 和骨折风险增加有关。NLR、PLR 和 SII 的对数转换每标准差增加,OP 风险的相应危险比和 95%置信区间(CI)分别为 1.113(1.093-1.132)、1.098(1.079-1.118)和 1.092(1.073-1.111),骨折风险的相应危险比和 95%CI 分别为 1.066(1.051-1.082)、1.059(1.044-1.075)和 1.073(1.058-1.089)。与非衰弱个体相比,衰弱前期和衰弱个体的 OP 风险分别增加 21.2%(95%CI:16.5-26.2%)和 111.0%(95%CI:98.1-124.8%),骨折风险分别增加 6.1%(95%CI:2.8-9.5%)和 38.2%(95%CI:30.7-46.2%)。系统性炎症水平与衰弱呈正相关,SII、NLR 和 PLR 的对数转换每标准差增加时,β(95%CI)分别为 0.034(0.031-0.037)、0.026(0.023-0.029)和 0.008(0.005-0.011)。衰弱表型部分介导了系统性炎症与 OP/骨折风险之间的关联。亚组和敏感性分析证实了这些发现的稳健性。
系统性炎症和衰弱表型与 OP 和骨折风险的增加独立相关。衰弱表型部分介导了系统性炎症与骨质疏松症特征之间的关联。这些结果强调了针对系统性炎症和衰弱进行干预在 OP 和骨折预防和管理中的重要性。